Temporomandibular Joint Disorders Question And Answers
Question 1. Enumerate causes of trismus (inability to open mouth) and describe myofacial pain dysfunction syndrome.
Or
Write Clinical features of myofacial pain dynfunction syndrome
Answer.
Myofacial Pain Dysfunction Syndrome
When muscle spasm develops, dysfunction as well as pain occurs and condition is designated as myofacial pain dysfunction syndrome.
Myofacial Pain Dysfunction Syndrome Etiology
- Abnormal occlusion: If occlusal contacts are painful and damaging, modification should be made by patient in pathway of closure. This can lead to strain and spasm of muscle which causes abnormal pressure on TMJ.
- Prosthetic disturbances: Faulty partial or complete dentures, overclosure, bilateral loss of molar teeth, etc. can lead to myofacial pain dysfunction syndrome.
- Orthodontic causes: Malocclusion can lead to myofacial pain dysfunction syndrome.
- Emotional causes: Obsessions such as over care of teeth, food habits can cause myofascial pain dysfunction syndrome.
- Tooth muscle theory: Interferences in occlusion leads to altered proprioceptive feedback which causes incoordination and spasm to muscles of mastication.
- Psychophysiologic theory: Spasm of muscles of mastication is responsible for myofacial pain dysfunction syndrome. Myospasm can lead to degenerative arthritis and contracture degenerative changes. Spasm is caused by:
- Dental restoration: By fixed and removable prosthesis which encroaches over space between the maxilla.
- Loss of tooth: Bilateral loss of posterior teeth can lead to overcontraction of muscle.
- Oral habit: They can lead to muscle fatigue.
- Denture irritation: Overhanging margins or maloccluding restorations.
- Joint Problem:
- Hypermobility caused by lax ligament can lead to TMJ dysfunction.
- Patient with steep angulations of articular eminence are more prone to TMJ dysfunction syndrome.
- Degenerative changes, secondary to chronic parafunctional habits or over closure is due to bilateral loss of molar teeth lead to myofacial pain dysfunction syndrome.
“Understanding TMJ disorders through FAQs: Q&A explained”
Read And Learn More: Oral Medicine Question And Answers
Myofacial Pain Dysfunction Syndrome Clinical Features
Myofacial Pain Dysfunction Syndrome Symptoms
- Middle age group is more commonly affected.
- Females are more commonly affected as compared to males.
- It occurs multiple times in any time of the day. Its frequency increased in emotional tension.
- Patient complaints of pain in mastication. Pain is restricted to preauricular area and is also radiated to temporal, frontal and occipital region.
- On mandibular movement patient complaints of sound on rubbing, grinding, clicking noise
- Patient can also complaint of tinnitus or toothache.
- At times, partial or complete hearing loss is present.
Temporomandibular Joint Dysfunction (TMD): Causes and Management
Myofacial Pain Dysfunction Syndrome Signs
Laskin’s four cardinal signs:
- unilateral pain: It is dull ache felt in ear or preauricular area or at angle of mandible.
- Muscle tenderness: Most frequent areas are neck of mandible and in region distal and superior to maxillary tuberosity.
- Clicking or popping noise in TMJ.
- Limitation of jaw function or deviation of mandible on opening.
Myofacial Pain Dysfunction Syndrome Management
Refer to Ans 2 of the same chapter.
Question 2. Write short note on management of myofacial pain dysfunction syndrome.
Answer.
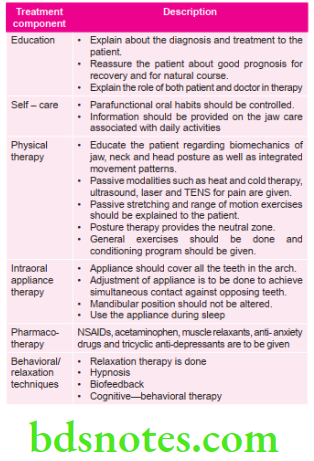
Myofacial Pain Dysfunction Syndrome Management
Counseling
- Re-educate the patient to the mechanism involved and factors causing or aggravating disorder.
- Reassure the patient about the benign character of the myospasm.
- Suggestion act as a powerful tool treatment.
Myofacial Pain Dysfunction Syndrome Muscle Relaxation Exercise
- Patient is told to keep his/her tongue as posteriorly as possible in contact with palate and mandible should be in retruded position. Tongue exercise is to be performed daily for 10 min.
- Patient is told to open his mouth slowly under the pain limit.
- Resistance is the technique based on the physiologic principle of reciprocal music inhibition, e.g. depressing mandible.
“Importance of studying TMJ disorders for better diagnostic outcomes: Questions explained”
Myofacial Pain Dysfunction Syndrome Pharmacotherapy
- Pain control is to be done by use of analgesics and the most commonly used is aspirin.
- Tranquilizers are used which have major calming effects.
- Antidepressants: Lithium carbonate and caffeine.
- Sedative are used.
- Hypnotic produces sleep and resemble as natural sleep.
Myofacial Pain Dysfunction Syndrome Biofeedback
- Most commonly used biofeedback device is electromyograph. This method elaborately gauges amperage and voltage. This method is non-invasive and painless.
- In temperature biofeedback, a delicate thermometer is placed over the skin. Higher the temperature, the high is the pitch of sound.
Myofacial Pain Dysfunction Syndrome Bruxism Prosthesis
- Soft mouth guard is used.
- Anterior occlusion prosthesis, i.e. Lucia jig and anterior bite plane are used.
- Mandibular posterior coverage: All posterior teeth of mandible should be covered, when jaw is closed.
- Complete maxillary or mandible coverage: All the occlusal surfaces of mandibular and maxillary arch should be covered. It provides grip to the teeth and act as a splint, it also prevents occluding tendency of posterior teeth
Myofacial Pain Dysfunction Syndrome Physical Medication
- Hot packs are given directly to trigger zones. Patient should place hot fermentation not less than 10 minutes. For this, woolen cloth soaked in hot water is preferable.
- Massage is done. Massage provides relief from muscle spasm.
- Diathermy and ultrasound: Reduces heat and improve local circulation.
- Electrical stimulation: Tetanizing and sinusoidal current is used. It leads to the breakage of muscle spasm. In this therapy electrodes should be kept over the painful areas and tetanizing current is given until the good contraction of affected muscle is obtained. Current should be given till tolerance level and beyond that. As tetanizing current is switched off the sinusoidal current is given until desired contraction is achieved.
- Oral myofunctional therapy: In this muscles of mouth are reeducated and face work in the proper balanced relationship. In this habit breaking is done, infant feeding is done, etc.
“Common challenges in diagnosing TMJ disorders effectively: FAQs provided”
Myofacial Pain Dysfunction Syndrome Anesthesia
- Trigger points: Local anesthetic should be injected at the painful trigger points. It permanently terminates pain. Local anesthetic solution should be used without vasoconstrictor.
- Refrigerated spray: Ethyl chloride is used which reduces the spasm of muscle by leading to counter irritation. It is sprayed at the trigger points in seeping motion.
Myofacial Pain Dysfunction Syndrome Other Therapies
- Hypnotherapy: Patient should have to co-operate with hypnotist. By this method at times, muscle relaxation is achieved.
- Acupuncture: It is a conservative pain control method. Under this method, needles are inserted in joints at meridian points. This therapy primarily is given to achieve relief from pain.
- Surgery: Surgical procedures such as eminectomy, zygomectomy, meniscectomy, High condylectomy with material interposed between articulating surfaces should be performed.
- Restorations: Faulty restorations should be removed. At times, full mouth rehabilitation should also be done for achieving centric occlusion.
- Prosthodontic therapy: Overclosure due to bilateral loss of posterior teeth can lead to pain in TMJ. In such cases normal vertical dimensions should be achieved by removable or fixed prosthesis.
- Orthodontic therapy: It is carried out in patients with crossbite, traumatic bite and in parafunctional habits.
- Orthognathic therapy: In patients with skeletal discrepancies which leads to malocclusion, this therapy is done.
“Why is early detection critical for managing TMJ disorders? Answered”
Question 3. Discuss TMJ anatomy. Classify TMJ disorder and discuss in detail myofacial pain dysfunction syndrome.
Answer.
Anatomy of TMJ
This is a synovial type of condylar variety joint, it consists of:
Articular Surfaces
- The upper articular surface is formed by the articular eminence and anterior part of mandibular fossa.
- The inferior articular surface is formed by head of mandible.
Articular Disk
The disk is an oval bulbous plate that divides the joint in upper and lower compartments. The upper compartment permit gliding movements and lower compartment permits rotatory as well as gliding movements.
Myofacial Pain Dysfunction Syndrome Ligaments
The ligaments are as follows:
- The fibrous capsule: It is a attached above to the articular tubercle, circumference of mandibular fossa and squamotympanic fissure and below the neck of mandible.
- The lateral ligament: It reinforces and strengthen the lateral part of capsular ligament. It is attached above to articular tubercle and below posterolateral aspect of neck of mandible.
- The sphenomandibular ligament: It is an accessory ligament which is attached superiorly to spine of sphenoid, and inferiorly to lingual of mandibular foramen.
- Stylomandibular ligament: It is also a accessory ligament of joint. It represents the thickened part of deep cervical fascia which separates parotid and submandibular salivary gland.
Myofacial Pain Dysfunction Syndrome Relations
- Lateral: Skin and fascia, parotid gland and temporal branch of facial nerve.
- Medial: Spine of sphenoid, auriculotemporal and chorda tympani nerves, middle meningeal artery.
- Anterior: Lateral pterygoid, masseteric nerve and vessels.
- Posterior: Superficial temporal nerves and auriculotemporal nerve.
- Superior: Middle cranial fossa and middle meningeal vessels.
- Inferior: Maxillary artery and nerve.
Classification of TMJ Disorders
- Developmental
- Agenesis of condyle.
- Hyperplasia of condyle.
- Traumatic
- Trauma to disk.
- Trauma to ligament.
- Subluxation or dislocation.
- Ankylosis.
- Trauma to muscle.
- Inflammatory
- Infective:
- Pyogenic infective.
- Syphilis.
- TB
- Actinomycosis.
- Osteomyelitis.
- Non-infective:
- SLE.
- Synovitis.
- Myositis.
- MPDS.
- Metabolic Disorders
- Gout.
- Chondrocalcinosis.
- Amyloidosis.
- Gaucher’s disease.
- Infective:
- Neoplasms
- Benign:
- Osteoma.
- Chondroma.
- Osteochondroma.
- Benign:
- Malignant
- Osteosarcoma.
- Chondrosarcoma.
- Malignant lymphoma.
- Neuropathic
- Charcoat Joint
- Internal derangement.
- Disk displacement.
- Charcoat Joint
- Disk fracture
For myofacial pain dysfunction syndrome, refer to Ans 1 and Ans 2 of the same chapter.
“Steps to explain causes of TMJ disorders: Bruxism vs trauma: Q&A guide”
Question 4. Write short note on TMJ ankylosis.
Answer. TMJ ankylosis is an abnormal immobility and consolidation of joint.
TMJ Ankylosis Classification
- True: It is a condition that produces fibrous or bony adhesion between the articular surfaces of TMJ.
- False: Results from pathologic conditions outside the joint, that results in mandibular mobility.
- Bony: Bone lies in between the articulating surfaces and prevent movements of bone.
- Fibrous: In this fibrous tissue hinders the movement of bone
- Partial: In this, there is incomplete union between articulating surfaces
- Complete: In this, complete union is prevent between articulating surfaces.
TMJ Ankylosis Etiology
- False
- Myogenic: Fibrosis caused by the chronic infection in elevator muscles of mastication.
- Neurogenic: Consists of brain tumor, epilepsy, etc.
- Psychogenic: Patient feels no pain and is unable to separate the jaws.
- Bone Impingement: Caused by impingement of coronoid process.
- Trauma: It leads to fibrous adhesions of soft tissues.
- True
- Congenital: It consists of congenital syphilis, birth injuries.
- Trauma: Trauma to chin, malunion of condylar fracture etc.
- Inflammatory: Inflammation of TMJ
- Others: Tissue loss along with scarring.
TMJ Ankylosis Clinical Features
- It is seen primarily in young age between 1 to 10 years.
- Pain and trismus which is related to duration of ankylosis.
- Oral problems, i.e. poor oral hygiene, carious teeth, periodontal problems and malocclusion.
- Unilateral ankylosis is more common than bilateral.
Clinical Features of Unilateral Ankylosis
- Seen in a child or in a person where the onset was usually in the childhood:
- Obvious facial asymmetry.
- Deviation of the mandible and chin on the affected side.
- The chin is receded with hypoplastic mandible on the affected side.
- Roundness and fullness of the face on the affected side.
- The appearance of flatness and elongation on the unaffected side.
- Lower border of the mandible on the affected side has a concavity that ends in a well-defined antegonial notch.
- In unilateral ankylosis, some amount of oral opening may be possible. Interincisal opening will vary depending on whether it is fibrous or bony ankylosis.
- Crossbite may be seen.
- Class 2 Angle malocclusion on the affected side plus unilateral posterior cross bite on the ipsilateral side seen.
- Condylar movements are absent on the affected side.
Clinical Features of Bilateral Ankylosis
- Patient has bird-face appearance.
- Gliding movements of TMJ are absent.
- Muscles of mastication get fibrosed.
- Patient has Class II malocclusion.
- There is presence of anterior open bite.
TMJ Ankylosis Management
- Brisement force: Forceful opening of mouth.
- Condylectomy: Removal of condyles is done.
- Gap arthroplasty: It is done at neck of mandible.
“Role of stress in causing TMJ dysfunction: Questions answered”
Question 5. Write short note on bruxism.
Answer. Bruxism is defined as clenching/grinding of teeth when the individual is not swallowing or chewing.
Bruxism Clinical Features
- Facet patterns are present.
- Bruxism occurring during rapid eye movement sleep is most damaging.
- Chronic bruxism may lead to sensitive worn-out, decayed, fracture, loose or missing teeth.
- Long-term bruxers experience jaw tenderness, jaw pain, fatigue of facial muscles, headache, neckache, earache and hearing loss.
- Bruxism may damage the TMJ.
- Malocclusion or bad bite is most common among bruxers.
- There may be loss of integrity in periodontal structures resulting in loosening or drifting of teeth and even gingival recession occurs.
Bruxism Etiology
- It occurs due to mild occlusal disturbances.
- Gastrointestinal disturbances or endocrine disturbances.
- Due to emotional tension.
- In occupations like watchmaker.
Bruxism Management
- Psychotherapy: Since main cause for the bruxism is stress, various psychotherapeutic approaches should be adapted. For example, listening of progressive relaxation or autosuggestion tapes before going to sleep.
- Wakeful EMG feedback: This is the psychological approach for reducing the stress. At the time of bruxing, relevant muscles become active and this activity is measured by electromyograph. In this patient should be asked to sit comfortably. Now one or more pair of recording electrodes attached to skin in close contact to appropriate muscles. Such electrodes transfer information about the muscle activity which is seen on computer screen. Instruct the patient to consciously lower the level below threshold line. By becoming alert to muscle tension, patient can develop the technique to decrease the tension, so there is decrease in bruxism
- Exercise: Isokinetic and the stretching exercises of mandible may help to reduce the bruxism.
- Drugs: Anti-anxiety drugs, muscle relaxants and other drugs provide symptomatic relief.
- Equilibration therapy: Bruxism is traceable to malocclusion, elimination of this cause is done by orthodontic adjustment.
- Splints: In this methods used are night guards, bite guards, occlusal splints, bite plates, removable appliances or interocclusal orthopedic appliances. Removable appliances should be worn in night.
Question 6. Write short note on Ely’s Cyst.
Answer. It is also known as subchondral cyst.
- These are very small areas of degeneration which are filled with fibrous tissue and are visible below the bony surface of mandibular condyle.
- These tiny radiolucent areas have slightly irregular borders and are less sharply defined.
- Some of these areas are surrounded by various areas of increased density which may be thin or they can be well defined and at times, they are relatively wide but are not sharply defined. These areas are cystic and are known as Ely’s cyst.
Question 7. Define pain. Give classification of orofacial pain. Describe etiology, clinical features and management of myofacial pain dysfunction syndrome.
Or
Define pain. Classify pain and describe in detail etiology, clinical features, differential diagnosis and management of myofacial pain dysfunction syndrome.
Or
Classify and defined orofacial pain. Write in detail about the etiology, clinical features, differential diagnosis and management of MPDS.
Or
Define pain. Write in detail about myofacial pain dysfunction syndrome.
Answer. Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage. By IASP (International association of study for pain).
Orofacial pain is an unpleasant emotional experience initiated by noxious stimuli and is transmitted over a specialized neural network to central nervous system, where it is interpreted as such.
TMJ Disorders: Key Questions on Diagnosis and Treatment Options
Classification of Orofacial Pain
- Superficial pain
- Mucogingival pain
- Cutaneous pain
- Deep pain
- Odontogenic pain:
- Pulpal pain
- Periodontal pain
- Odontogenic pain:
- Musculoskeletal pain:
- Muscle pain:
- Neoplastic myofascial pain
- Muscle-splinting pain
- Muscle spasm pain
- Local muscle soreness
- TMJ pain
- Capsule pain
- Disc attachment pain
- Retrodiscal pad pain
- Arthography pain
- Soft connective tissue pain
- Osseous pain.
- Muscle pain:
- Vascular pain:
- Atypical facial neuralgia
- Cranial arteritis
- Visceral pain:
- True visceral pain
- Reflex sympathetic dystrophy
Neurogenous pain
- Traumatic neuroma pain:
- Neuritis pain:
- Peripheral neuritis
- Herpes zoster
- Neuralgia pain:
- Idiopathic neuralgia
- Symptomatic neuralgia
- Neuritis pain:
- Psychogenic pain:
- Pschycogenic intensification pain
- Delusional pain
- Conversion hysteria pain
Myofacial Pain Dysfunction Syndrome Differential Diagnosis
- Giant cell arteritis (temporal arteritis).
- Cardiac pain (angina and acute coronary syndromes) can radiate to the neck and jaw, but is usually more acute.
- Dental problems.
- Trigeminal neuralgia.
- Migraine and other causes of headache.
- Herpes zoster.
- Other ENT disorders, e.g. salivary gland disorders and ENT neoplasms.
The location of the pain helps in diagnosis. The pain in
TMDs is centred immediately in front of the tragus of the ear and projects to the ear, temple, cheek and along the mandible.
For etiology, clinical features refer to Ans 1 and management of myofacial pain dysfunction syndrome refer to Ans 2 of same chapter.
TMJ Disorders: Key Questions on Diagnosis and Treatment Options
“How does arthritis contribute to TMJ disorders? FAQ explained”
Question 8. Write short note on clinical features of ankylosis of TMJ.
Answer. Following are the clinical features of ankylosis of TMJ.
Unilateral Ankylosis of TMJ
- Patient is unable to open the mouth. But on forceful opening mouth can be opened to several millimeters.
- Face becomes asymmetrical.
- Patient’s face gets deviated towards the affected side.
- Midline shift is present.
- Crossbite is present.
Bilateral Ankylosis of TMJ
- Presence of bird-face appearance
- Class 2 malocclusion is seen
- Incisors are protruded
- Anterior open bite is present
- Micrognathia is present
- Convex profile is present
- Thyromental angle is reduced
- Double chin is present
- Teeth are impacted or submerged
- No gliding movement is present.
- Since bilateral ankylosis is present, jaw movements are restricted.
- Due to poor oral hygiene, dental caries and periodontal diseases are present.
Question 9. Classify TMJ disorders. Discuss, etiology, clinical features, investigations, management of myofacial pain dysfunction syndrome.
Or
Enumerate TMJ disorders. Describe clinical features, investigations and management of MPDS (Myofascial pain dysfunction syndrome)
Answer. For classification of TMJ disorders, refer to Ans 3 of same chapter.
For etiology and clinical features of myofacial pain dysfunction syndrome refer to Ans 1 of same chapter.
For management of myofacial pain dysfunction syndrome, refer to Ans 2 of same chapter.
Investigations
- Based on clinical examination Laskin’s four cardinal signs are sufficient to investigate and give proper diagnosis:
- Laskin’s four cardinal signs:
- unilateral pain: It is dull ache felt in ear or preauricular area or at angle of mandible.
- Muscle tenderness: Most frequent areas are neck of mandible and in region distal and superior to maxillary tuberosity.
- Clicking or popping noise in TMJ.
- Limitation of jaw function or deviation of mandible on opening.
- Radiograph shows no relevant changes.
- On palpation of TMJ from external auditory meatus, there is no tenderness present.
“Early warning signs of issues addressed by understanding TMJ disorder pathogenesis: Common questions”
Question 10. Write in brief on clinical features of unilateral ankylosis.
Answer.
Clinical Features of Unilateral Ankylosis
Seen in a child or in a person where the onset was usually in the childhood:
- Obvious facial asymmetry.
- Deviation of the mandible and chin on the affected side.
- The chin is receded with hypoplastic mandible on the affected side.
- Roundness and fullness of the face on the affected side.
- The appearance of the flatness and elongation on the unaffected side.
- The lower border of the mandible on the affected side has a concavity that ends in a well-defined antegonial notch.
- In unilateral ankylosis, some amount of oral opening may be possible. Interincisal opening will vary depending on whether it is fibrous or bony ankylosis.
- Crossbite may be seen.
- Class 2 Angle malocclusion on the affected side plus unilateral posterior crossbite on the ipsilateral side seen.
- Condylar movements are absent on the affected side.
“Asymptomatic vs symptomatic effects of ignoring TMJ triggers: Q&A”
Question 11. Write short note on MPDS.
Or
Write short answer on myofacial pain dysfunction syndrome.
Answer. When muscle spasm develops, dysfunction as well as pain occurs and condition is designated as myofacial pain dysfunction syndrome.
Etiology
- Abnormal occlusion: If occlusal contacts are painful and damaging, modification should be made by patient in pathway of closure. This can lead to strain and spasm of muscle which causes abnormal pressure on TMJ.
- Prosthetic disturbances: Faulty partial or complete dentures, overclosure, bilateral loss of molar teeth, etc. can lead to myofacial pain dysfunction syndrome.
- Orthodontic causes: Malocclusion can lead to myofacial pain dysfunction syndrome.
- Emotional causes: Obsessions such as over care of teeth, food habits can cause myofascial pain dysfunction syndrome.
- Tooth muscle theory: Interferences in occlusion leads to altered proprioceptive feedback which causes incoordination and spasm to muscles of mastication.
Myofacial Pain Dysfunction Syndrome Clinical Features
Myofacial Pain Dysfunction Syndrome Symptoms
- Middle age group is more commonly affected.
- Females are more commonly affected as compared to males.
- It occurs multiple times in any time of the day. Its frequency increased in emotional tension.
- Patient complaints of pain in mastication. Pain is restricted to preauricular area and is also radiated to temporal, frontal and occipital region.
- On mandibular movement patient complaints of sound on rubbing, grinding, clicking noise
- Patient may also complaint of tinnitus or toothache.
- At times, partial or complete hearing loss is present.
Myofacial Pain Dysfunction Syndrome Signs
Laskin’s four cardinal signs:
- unilateral pain: It is dull ache felt in ear or preauricular area or at angle of mandible.
- Muscle tenderness: Most frequent areas are neck of mandible and in region distal and superior to maxillary tuberosity.
- Clicking or popping noise in TMJ.
- Limitation of jaw function or deviation of mandible on opening.
“Differential applications of myofascial pain vs disc displacement: Questions answered”
Myofacial Pain Dysfunction Syndrome Diagnosis
Based on clinical examination Laskin’s four cardinal signs are sufficient to investigate and give proper diagnosis:
Myofacial Pain Dysfunction Syndrome Laskin’s Four Cardinal Signs:
- unilateral pain: It is dull ache felt in ear or preauricular area or at angle of mandible.
- Muscle tenderness: Most frequent areas are neck of mandible and in region distal and superior to maxillarytuberosity.
- Clicking or popping noise in TMJ.
- Limitation of jaw function or deviation of mandible on opening.
- Radiograph shows no relevant changes.
- On palpation of TMJ from external auditory meatus, there is no tenderness present.
Myofacial Pain Dysfunction Syndrome Treatment
Leave a Reply