Surgical Anatomy Of The Parotid Gland And Management Of Pleomorphic Adenoma
Question 1. Describe the surgical anatomy of the parotid gland. Describe signs, symptoms, and management of pleomorphic adenoma of the parotid gland.
Answer. The parotid gland is a major salivary gland.
Surgical Anatomy of Parotid Gland
- The parotid gland lies beneath the skin, in front, and below the ear. The parotid gland is contained in the investing layer of the deep fascia of the neck, which is known as the parotid fascia.
- The parotid gland is separated from the submandibular gland by a fascial thickening known as the stylomandibular ligament.
- Parotid space is occupied by the parotid gland.
- From the anterolateral edge of the gland, the parotid duct or Stensen’s duct passes lateral to the masseter muscle.
- The parotid duct turns medial at the anterior margin of the muscle, where it is related to the buccal fat pad or “boule de Bichat.”
“Comprehensive Overview Of Pleomorphic Adenoma Symptoms”
- The location of the buccal pad is medial to the parotid duct, between the masseter and buccinator muscles.
- Stenson’s duct pierces the buccinator muscle and enters the oral cavity at the level of the upper second molar tooth.
- At times, accessory parotid tissue may extend along the stenson’s duct. A short accessory duct may enter the main duct.
Read And Learn More: General SurgeryQuestions and Answers.
“Can Pleomorphic Adenoma Cause Facial Nerve Damage”
Parotid gland Parotid Fascia
- Parotid fascia is mainly the splitting of the f general investing layer, which envelops both the parotid and submandibular glands, forming the superficial and deep layers.
- Superficial layer is dense, and thin,gh while the deep layer is thin and The stylomandibularlar ligament,t which lies between the styloid process and the angle of the mandible, le, is derived from the deep layer.
- The ligament is tough and separates the parotid from the submandibular gland.
- Communication of parotid space is medial with the lateral pharyngeal space and with the posterior area of the masticator space.
- The posterior area of the masticator space consists of the masseter muscle, pterygoid muscles, the small pterygomandibular space, and the space of the body of the mandible.
- As many intraparotid anatomic structures radiate from the parotid gland, the surgeon should be familiar with all those structures, especially those that should not be sacrificed.
“The Role Of Imaging Tests In Parotid Gland Tumor Diagnosis”
Bed of the Parotid Gland
Complete removal of the parotid gland reveals the following structures:
- Internal jugular vein, i.e., one vein
- Carotis externa artery and carotiinternalna artery, i,.e. two arteries
- IX, X, XI, and XII cranial nerves, i.e. four nerves
“What Tests Confirm A Pleomorphic Adenoma Diagnosis”
Parotid gland Signs and Symptoms (Clinical Features)
- Middle-aged women around 40 years old are commonly affected.
- Swelling is painless.
- Parotid swelling has the following classical features:
- It presents as a swelling in front, below, and behind the ear.
- Raises ear lobule.
- The retromandibular groove is obliterated.
“Best Practices For Parotid Gland Tumor Surgical Management”
- It is rubbery or firm
- Soft area indicates necrosis
- In long-standing cases, it can be hard surface can be nodular
- Skin is stretched and becomes shiny
- Being a benign tumor, it is neither adherent to the skin nor the masseter.
- After a few years, pleomorphic adenoma shows features of transformation into malignancy.
Parotid gland Management
- Surgery is the first of e-management.
- If only the superficial lobe is involved, then superficial parotidectomy is done wherein the parotid superficial to the facial nerve is removed.
- Various steps in superficial parotidectomy:
“Effective Ways To Manage Parotid Gland Surgery Recovery“
- Give incision: the incision should start in front of the tragus, vertically descend downwards, curve around the ear lobule, the mastoid process, and be carried to the neck.
- The facial nerve should be recognized, which lies 1cm inferomedial to the pointed end of the tragal cartilage of the external ear.
- Trace the posterior belly of the digastric till the mastoid process.
- The facial nerve lies between the muscle and the tympanic plate.
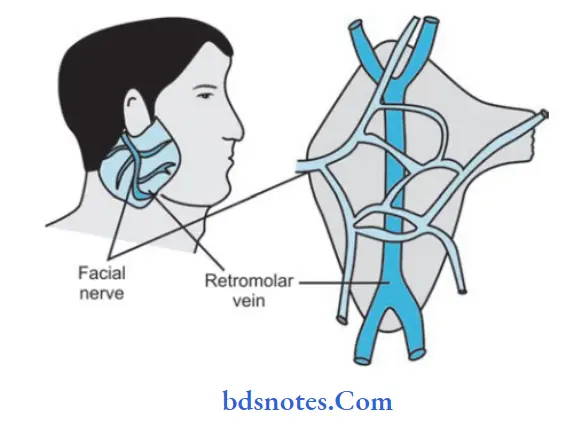
- Both the facial nerve and retromandibular vein divide the parotid gland into deep and superficial lobes. Benign tumors do not invade the faciovenous plane of Patey.
- Gentle handling, good suction, and nice hemostasis provide visibility tothe rve.
- The tumor, along with the lobe, should be removed in Toto to avoid spillage.
- If both the lobes aare involvedd then total conservative parotidectomy is done.
- In this, tumor, along with the normal lob,e is removed by retaining the g facial nerve. Avoid rupture of the gland.
Leave a Reply