Periodontal Restorative Inter Relationships
Question 1. What is periodontal restorative interrelationships and its rationale? Explain in detail.
Answer.
Periodontal-restorative Inter-relationships
“Role of counseling in explaining benefits of interdisciplinary care”
The relationship between periodontal health and the restoration of teeth is intimate and inseparable. For restorations to survive longterm, the periodontium must remain healthy so that the teeth are maintained. For the periodontium to remain healthy, restorations must be critically managed in several areas so that they are in harmony with their surrounding periodontal tissues. To maintain or enhance the patient’s esthetic appearance, the tooth/tissue interface must present a healthy natural appearance, with gingival tissues framing the restored teeth in a harmonious manner.
“Understanding the role of periodontal health in restorative dentistry”
Read And Learn More: Periodontics Question And Answers
Rationale
- Periodontal treatment is undertaken to ensure the establishment of stable gingival margins before tooth preparation. Noninflamed, healthy tissues are less likely to change as a result of subgingival restorative treatment or postrestoration periodontal care. In addition, tissues that do not bleed during restorative manipulation allow for a more predictable restorative and esthetic result.
- Certain periodontal procedures are designed to provide for adequate tooth length for retention, access for tooth preparation, impression making, tooth preparation, and finishing of restorative margins in anticipation of restorative dentistry. Failure to complete these procedures before restorative care can add to the complexity of treatment and introduce unnecessary risk of failure.
- Periodontal therapy should antecede restorative care because the resolution of inflammation may result in the repositioning of teeth or in soft tissue and mucosal changes. Failure to anticipate these changes may interfere with prosthetic designs planned or constructed before periodontal treatment.
“Importance of studying restorative-periodontal interrelationships for dental professionals”
- Traumatic forces placed on teeth with ongoing periodontitis may increase tooth mobility discomfort, and possibly the rate of attachment loss. Restorations constructed on teeth free of periodontal inflammation, synchronous with a functionally appropriate occlusion, are more compatible with long-term periodontal stability and comfort.
- Quality, quantity, and topography of the periodontium may play important roles as structural defense factors in maintaining periodontal health. Orthodontic tooth movement and restorations completed without the benefit of periodontal treatment designed for this purpose may be subject to negative changes that complicate construction and future maintenance.
- Successful esthetic and implant procedures may be difficult or impossible without the specialized periodontal procedures developed for this purpose.
Question 2. Write short answer on biological width.
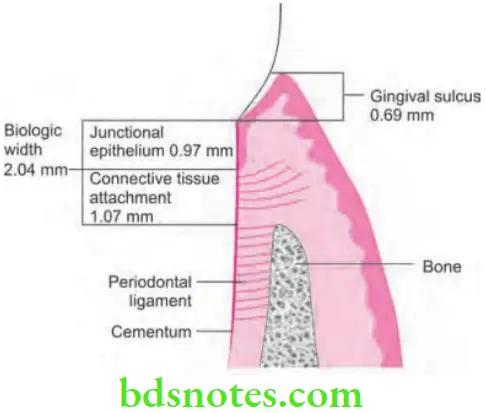
Answer. Biologic width is the circumferential rim of space around teeth where the junctional epithelium and the underlying connective tissue of the gingiva attach to the teeth.
- Invasion into the biologic width is avoided to prevent attachment los and persistent gingival inflammation
- Biologic width is junctional epithelium 0.97 mm + connective tissue attachment 1.07 mm = 2.04 mm
“Common challenges in managing restorative-periodontal interrelationships”

“Why is interdisciplinary care critical for restorative-periodontal success?”
Evaluation of Biologic Width
- Radiographic interpretation can identify interproximal violations of biologic width. But with the more common locations over mesiofacial and distofacial line angles of teeth, radiographs are not diagnostic due to tooth superimposition.
- A more positive assessment can be done clinically by measuring distance between bone and the restoration margin by using a sterile periodontal probe. Push the probe through the anesthetized attachment tissues from the sulcus to underlying bone. If this distance is less than 2 mm at one or more locations, diagnosis of biologic width violation can be confirmed. This assessment is completed circumferentially around the tooth to evaluate the extent of problem. However, biologic width violations can occur in some patients in whom the margins are located more than 2 mm above the alveolar bone level.
“Asymptomatic vs symptomatic effects of misaligned treatment goals”
- Biologic, or attachment width can be identified for the individual patient by probing to the bone level (referred to as “sounding to bone”) and subtracting the sulcus depth from the resulting measurement. This measurement must be done on teeth with healthy gingival tissues and should be repeated on more than one tooth to ensure an accurate assessment.
- The technique allows the variations in sulcus depths found in individual patients to be assessed and factored into the diagnostic evaluation.
“Steps to create a treatment plan integrating periodontal and restorative care”
“Role of periodontal evaluation in restorative treatment planning”
Correction of Biologic Width Violations
- Biologic width violations can be corrected either by surgically removing bone away from proximity to restoration margin or by orthodontically extruding the tooth and thus moving the margin away from the bone.
- Surgery is the more rapid of the two treatment options. It is also preferred if the resulting crown lengthening creates a needed tooth length.
- If the biologic width violation is on inter – proximal side, or if the violation is across the facial surface and the gingival tissue level is correct, orthodontic extrusion is indicated.
- Orthodontic procedure can be accomplished by two ways i.e.
- By slow orthodontic extrusive force: Here, tooth gets extruded slowly which bring bone and gingival tissue with it.
- By rapid orthodontic extrusive force: Here tooth extrusion is to the desired amount and is carried for several weeks.
“Early warning signs of poor periodontal-restorative alignment”
Biological Width Clinical Significance
- When restoring teeth, if the margins of the restorations violate the biologic width, gingival inflammation ensues.
- If left untreated, it can lead to bone loss.
- Crown lengthening is a surgical procedure that is performed clinically (i.e., before restoration delivery) to intentionally create space for the biologic width to reestablish.
Leave a Reply