Resective Osseous Surgery
Answer. Osseous defects are those defects, which are formed as a result of destruction of alveolar bone due to periodontal disease.
Osseous surgery: Osseous surgery may be defined as the procedure by which changes in the alveolar bone can be accomplished to rid it of deformities induced by the periodontal disease process or other related factors, such as exostosis and tooth supraeruption.
“Understanding the role of resective osseous surgery in periodontics”

“Importance of studying resective osseous surgery for dental professionals”
Resective Osseous Surgery
It is the procedure designed to restore the form of preexisting alveolar bone to the level existing at the time of surgery or slightly more apical to this level is known as resective osseous surgery.
Resective Osseous Surgery Objectives
- Removal of osseous defects
- Correction of bone morphology
- To create harmonious relation between gingiva and alveolar bone by eliminating periodontal pockets.
- To create a favorable postoperative gingival morphology
“Common challenges in performing resective osseous surgery”
Read And Learn More: Periodontics Question And Answers
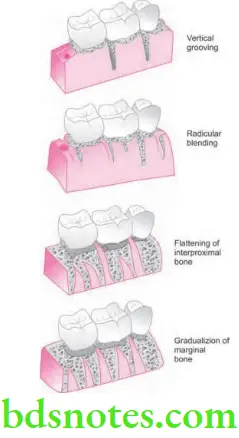
Steps in Resective Osseous Surgery
Following are the steps which are suggested for the respective osseous surgery:
- Vertical grooving
- Radicular blending
- Flattening inter proximal bone
- Gradualizing marginal bone
“Steps to perform resective osseous surgery effectively”
“Role of osteoplasty and ostectomy in resective osseous surgery”
Vertical Grooving
- Vertical grooving is carried out to reduce the thickness of the alveolar housing as well as to provide relative prominence to the radicular aspects of teeth.
- It gives continuity from the interproximal surface onto the radicular surface.
- This is the first step of the resective process as it can define the general thickness and subsequent form of the alveolar housing.
- Vertical grooving should be performed with rotary instruments, such as round carbide burs.
- Advantages of vertical grooving are most apparent with thick bony margins, shallow crater formations, or other areas that require proximal osteoplasty and minimal ostectomy.
- It is contraindicated in areas with close roots or thin alveolar housing is present.
“Early warning signs of complications during surgery”
Radicular Blending
- It is the second step of the osseous resective technique and is an extension of vertical grooving procedure.
- Radicular blending is an attempt to visualize the bone over the entire radicular surface to give the best results from vertical grooving.
- This gives a smooth, blended surface for good flap adaptation.
- Radicular blending is necessary if vertical grooving is very minor or if the radicular bone is thin or fenestrated.
- Vertical grooving and radicular blending are osteoplastic techniques that do not remove supporting bone.
- Shallow crater formation, thick osseous ledges of bone in the radicular surfaces and class I and early class II furcation involvements are treated almost entirely with these two steps.
“Asymptomatic vs symptomatic effects of improper bone reshaping”
Flattening of Inter-proximal Bone
- Flattening of the interdental bone requires the removal of very small amounts of supporting bone.
- It is indicated when interproximal bone levels vary horizontally.
- Most of the indications for this step are one-walled interproximal defects or hemiseptal defects.
- Omission of flattening in such cases results in increased pocket depth on the most apical side of the bone loss.
- Flattening of interdental bone is not necessary with interproximal crater formations or flat interproximal defects.
- This procedure is best used in defects which are coronally placed, one-walled edge of a predominantly three-walled angular defect, and it can be helpful in obtaining good flap closure and improved healing in the three-walled defect.
- Limitation of this step is with resective osseous surgical therapy in general, is in the treatment of advanced lesions.
- Large hemiseptal defects would require removal of inordinate amounts of bone to provide a flattened architecture, compromised osseous architecture is the only logical solution.
“Steps to educate patients about resective osseous surgery benefits”
Gradualizing Marginal Bone
- Final step in osseous resection technique is an ostectomy process.
- Removal of bone is minimal but necessary to provide a sound, regular base for the gingival tissue to flow.
- Failure to remove small bony discrepancies on the gingival line angles allows the tissue to rise to a higher level than the base of the bone loss in interdental area. This leads to the process of selective recession and subsequent pocket reduction incomplete.
- This step of the procedure also requires gradualization and blending on the radicular surface.
- Both osteotomy procedures should be performed with proper care so as not to produce nick or grooves on the roots.
- When radicular bone is thin, it is extremely easy to overdo this step.
- In various hand instruments, such as chisels and curettes, are preferable to rotary instruments for gradualizing marginal bone.
“Role of counseling in explaining the importance of bone reshaping”
Placement of Flap and Closure
- After the completion of osseous resection, the clinician positions and sutures the flaps.
- Flaps can be replaced at their original position, to cover the new bony margin, or they may be apically positioned.
- Replacing the flap in areas that previously had deep pockets may result initially in greater postoperative pocket depth.
- Positioning the flap apically to expose marginal bone is one method of altering the width of the gingiva. However, such flap placement results in more postsurgical resorption of bone and patient discomfort than of the newly created bony margin which was covered by the flap.
- Positioning the flap to cover the new margin minimizes postoperative complications and results in optimal postsurgical pocket depths.
- Suturing may be accomplished using a variety of different suture materials and suture knots.
- The sutures should be placed with minimal tension to approximate the flaps, prevent their separation, and maintain the position of the flaps.
“How do educational materials clarify complex surgical procedures?”
Postoperative Maintenance
- Remove the non resorbable sutures such as silk after l week of healing. Some of the newer synthetic materials can be left up to 3 weeks or longer.
- During suture removal the periodontal dressing, if present, should be removed, and the surgical site is gently cleansed of debris by cotton pellet dampened with saline.
- After suture removal is done, the surgical site is examined carefully, and any of the excessive granulation tissue is removed by sharp curette.
- For maintenance of the surgical site in a plaque-free state, provide the patient with postsurgical maintenance instructions.
“Early warning signs of knowledge gaps in patient understanding”
- Chlorhexidine digluconate can be a valuable adjunct to postsurgical maintenance.
- A second postoperative visit should be kept at second or third week, and during the visit surgical site is lightly debrided for good results.
- Professional prophylaxis for complete plaque removal should be done every 2 weeks until healing is complete or the patient is maintaining appropriate levels of plaque control.
- Before starting with dental restorations, it is advisable to wait for at least 6 weeks postoperatively.
Leave a Reply