Pyramidal And Extrapyramidal Tracts
Describe the corticospinal (pyramidal) tract in brief and discuss its applied anatomy.
Answer. The pyramidal tract is a motor tract consisting of both corticospinal and corticonuclear tracts. However, conventionally it refers to only the corticospinal tract.
“Understanding The Role Of Pyramidal Tracts In Voluntary Movement”
Corticospinal (Pyramidal) Tract Origin, Course, And Termination
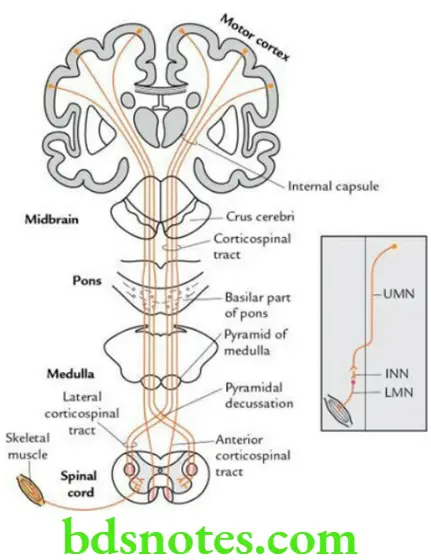
- Most of the fibers of the pyramidal tract arise from pyramidal cells of motor and premotor areas (areas 4 and 6) of the cerebral cortex.
- These fibers descend and traverse the following parts of the CNS in succession, viz. corona radiata, internal capsule (anterior two-thirds of the posterior limb and genu), crus cerebri (middle three-fifth), basilar part of pons and pyramid of the medulla.
“Importance Of Pyramidal And Extrapyramidal Tracts In Motor Control”
Read And Learn More: Selective Anatomy Notes And Question And Answers
Note that after emerging from pons, they condense to form pyramid-shaped bundles in the upper part of the medulla oblongata.
In the lower part of the medulla oblongata, about 70%–80% of fibers of the pyramidal tract cross to the opposite side and then descend in the lateral white column of the spinal cord on the opposite side as lateral corticospinal/crossed pyramidal tract and terminate on the anterior horn cells.
About 20%–30% of fibers of the pyramidal tract do not cross to the opposite side and descend in an uncrossed pyramidal tract/anterior corticospinal tract in the anterior white column of the spinal cord of the same side. These fibers finally also cross to the opposite side and terminate on the anterior horn cells.
“Risk Factors For Damage To Pyramidal And Extrapyramidal Tracts”
“Early Signs Of Issues With Pyramidal And Extrapyramidal Tracts”
Corticospinal Tract Function
The pyramidal tract is concerned with voluntary movements of the body.
Corticospinal Tract Applied anatomy
Lesion of pyramidal tract: It produces upper motor neuron (UMN) type of paralysis.
If the lesion is above the level of motor decussation, it causes spastic paralysis on the opposite side of the body, i.e. contralateral hemiplegia; while if the lesion is below the level of motor decussation, it leads to ipsilateral hemiplegia.
- Effects of upper and lower motor neuron type of paralysis: The lesions of upper motor neurons (UMNs) lead to:
- Spasticity paralysis
- Increased muscle tone
- Exaggeration of tendon reflexes
- No wasting of muscles except disuse atrophy.
“Role Of Extrapyramidal Tracts In Involuntary Movements”
The above signs and symptoms occur due to the hyperactivity of LMNs, as the control of UMNs on LMNs is lost.
The lesions of lower motor neurons (LMNs) lead to:
- Flaccid paralysis
- Decreased muscle tone
- Loss of tendon reflexes
- Wasting of muscle i.e. muscle atrophy
All these signs and symptoms occur due to the loss of nerve supply of the muscle.
Leave a Reply