Understanding Oral Cancer: Causes, Symptoms, and Treatment Options
Question 1. Describe the etiology, pathology, clinical features, and treatment of oral cancer.
Or
Describe the etiological factors, clinical features, and management of oral carcinoma.
Answer.
Etiology
Etiological Factors Of Oral Cancer
Tobacco smoking:
- Cigarettes
- Bidis
- Pipes
- Cigars
- Reverse smoking.
Use of smoking tobacco:
- Snuff dipping
- Tobacco sachets
- Tobacco chewing:
- Betal chewing
- Chewing of areca nut
- Consumption of alcohol
- Diet and nutrition: Vit. A, B complex, and C deficiency.
“Effective Ways To Manage Oral Cancer Pain At Home”
Read And Learn More: General Surgery Questions and Answers
Dental factors:
- Chronic irritation from broken teeth.
- Ill-fitting or broken prosthesis.
Ultraviolet radiation: Actinic radiation
Viruses:
- Herpes simplex virus
- Human papilloma virus
- Human immunodeficiency virus (HIV)
- Epstein-Barr virus
Immunosuppression:
- AIDS
- Organ transplantation
Chronic infection:
- Candidiasis
- Syphilis.
Occupational hazards: Woollen textile workers.
“Best Practices For Oral Cancer Prevention“
Genetic factors:
- Oncogenes
- Tumor suppressor genes
Pre-existing oral disease:
- Oral lichen planus
- Oral sub-mucous fibrosis
- Leukoplakia.
Oral Cancer Clinical Features
- Male predilection is seen.
- Carcinoma mostly occurs in older age.
- Site: Most commonly involved are the posterior and lateral borders of tongue and lower lip and less frequently the flor of mouth, palate and buccal mucosa.
- Small lesion is asymptomatic.
- Large lesion may cause some pain or paresthesia and swelling.
- Patients complain of persistent ulcer in the oral cavity.
- Function of organ is impaired.
- Appearance: The clinical appearance of a carcinomatous ulcer is that one of irregular shape induration and raised everted edges.
- Base: Usually have broad base and are dome like or nodular.
- Surface: May range from granular to pebbly to deeply creviced.
- Surface may be entirely necrotic and have ragged whitish gray appearance.
- Color: It may be completely red or red surface may be sprinkled with white necrotic or keratin area.
- Lymph nodes: Superficial and deep cervical nodes are commonly affected.
“The Role Of Tobacco And Alcohol In Oral Cancer Development“
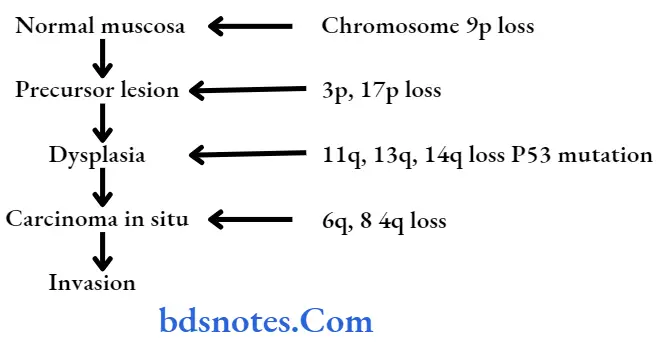
Oral Cancer Pathology
- Allelic imbalance (loss of heterozygosity [LOH]) has been identifid in tumor suppressor gene.
- Damage to tumor suppressor genes may also involve damage to other genes involved in growth control, mainly those involve in cell signaling (oncogenes, especially some on chromosome 11 and chromosome 16)
- Changes in oncogenes can disrupt cell growth control, leading ultimately to uncontrolled growth of cancer.
“Comprehensive Overview Of Oral Cancer Symptoms“
Management Of Oral Cancer
Management should be curative or palliative:
Early growth without bone involvement
- Curative radiotherapy using cesium needles or iridium wires, i.e. brachytherapy.
- Other option is wide excision wire 1–2 cm clearance.
Often, the approach to the tumor is by raising the cheek flp (outside). After the wide excision, the flap is placed back (Patterson operation). - Presently advanced technology in radiotherapy facilitates the use of external radiotherapy also.
The incidence of dreaded complications like osteoradionecrosis mandible has been reduced due to better radiotherapy methods. - Growth with mandible involvement: Here along with wide excision of the primary tumor hemimandibulectomy or segmental resection of the mandible or marginal mandibulectomy (using a rotary electric saw) is done.
- Operable growth with mandible involvement and mobile lymph nodes on the same side (confirmed by FNAC):
Along with wide excision ofthe primary, hemimandi bulectomy and radical neck lymph node dissection are done (commando operation).
Wide excision of the primary lesion, hemimandibulectomy with radical neck node dissection is called composite resection. - Operable growth with mandible involvement; mobile lymph node on the same side and opposite side: Along with wide excision of the tumor, Hemi-mandibulectomy, radical neck lymph node dissection on the same side, and functional block dissection on the opposite side are done, retaining the internal jugular vein, sternomastoid and spinal accessory nerve.
- Operable primary tumor with mobile lymph nodes on the same side but without mandibular involvement: Wide excision of the primary tumor and radical neck lymph node dissection on the same side are done. The mandible is not removed.
- Fixed primary tumor or advanced neck lymph node secondaries:
Only palliative external radiotherapy is given to palliate pain foundation and to prevent anticipated torrential hemorrhage. - Preoperative radiotherapy is often used in field lymph nodes to downstage the disease to make it operative.
- Postoperative radiotherapy is given in T3 and T4 tumors: N2 and N3 nodal status to reduce the recurrence and to improve the prognosis.
- Prophylactic block dissection has become popular in No no-diseases
- If growth is extending to the upper alveolus: Partial maxillectomy or total maxillectomy is done.
Oral Cancer Reconstruction After Surgery
Flaps used for reconstruction after oral surgery:
- Forehead flap based on the superficial temporal artery.
- Deltopectoral flip based on 1, 2, and 3 perforating vessels from internal mammary vessels.
- Pectoralis major myocutaneous flap (PMMF) based on the thoracoacromial artery.
- Free microvascular flaps may be from the radial artery forearm flap.
- For small defects—tongue flap, buccal flap, palatal mucoperiosteal flap.
Oral Cancer Chemotherapy
- Drugs used are methotrexate, cisplatin, vincristine, bleomycin, and adriamycin.
Often it is given intra-arterially through the external carotid artery using an arterial pump or by increasing the height of the drip more than l3 feet, to attain a pressure more than systolic pressure.
“Step-By-Step Guide To Diagnosing Oral Cancer”
- Chemotherapy can also be given IV or orally postoperatively.
- Initial chemotherapy to downstage the tumor followed by surgery and later again ends with chemotherapy.
- Chemoradiotherapy is used in unresectable tumors as consecutive therapy.
Oral Cancer Radiotherapy
- Early lesions are managed by radiotherapy.
- Radiotherapy is of two types, i.e. external radiotherapy and interstitial radiotherapy.
- In external radiotherapy large doses of 6000 to 8000 cGy units are given, i.e. 200cGy units/day
- Interstitial radiotherapy is indicated in infiltrating small lesions. Cesium 137 or iridium wires are placed within the tumor.
Minimal tissue resection is the basic advantage of this procedure.
Leave a Reply