Odontogenic Tumors Important Question And Answers
Question.1.Classify odontogenic tumors. Describe pathogenesis, histopathology, clinical features, and radiographic appearance of ameloblastoma.
Or
Classify odontogenic tumors describe in detail ameloblastoma of mandible.
Or
Describe in detail ameloblastoma.
Or
Describe in detail about clinical, radiographic, histopathological features of ameloblastoma.
Or
Classify odontogenic tumors and write in detail about ameloblastoma.
Or
Classify odontogenic tumor and describe the clinical features, radiographic features and histological features of ameloblastoma.
Or
Classify odontogenic tumor. Describe in detail the clinical features, histopathology, and treatment of ameloblastoma.
Odontogenic tumors
Answer.
Classification of Odontogenic Tumors By WHO (2017)
- Odontogenic carcinomas
- Ameloblastic carcinoma
- Primary intraosseous carcinoma, NOS
- Sclerosing odontogenic carcinoma
- Clear cell odontogenic carcinoma
- Ghost cell odontogenic carcinoma
“Understanding odontogenic tumors through FAQs: Q&A explained”
Odontogenic Tumors Important Questions And Answers
- Odontogenic carcinosarcoma
- Odontogenic sarcomas
- Benign epithelial odontogenic tumors
- Ameloblastoma
- Ameloblastoma, unicystic type
- Ameloblastoma, extraosseous/peripheral type
- Metastasizing ameloblastoma
- Squamous odontogenic tumor
- Calcifying epithelial odontogenic tumor
- Adenomatoid odontogenic tumor
- Ameloblastoma
“Importance of studying odontogenic tumors for better diagnostic outcomes: Questions explained”
Read And Learn More: Oral Pathology Question And Answers
- Benign mixed epithelial & mesenchymal odontogenic
tumors- Ameloblastic fibroma
- Primordial odontogenic tumor
- Odontoma
- Odontoma, compound type
- Odontoma, complex type
- Dentinogenic ghost cell tumor
- Benign mesenchymal odontogenic tumors
- Odontogenic firoma
- Odontogenic myxoma/myxofiroma
- Cementoblastoma
- Cemento-ossifying firoma
“Common challenges in diagnosing odontogenic tumors effectively: FAQs provided”
Classification of odontogenic tumors
Odontogenic Tumors Mcqs With Answers
Ameloblastoma
Pathogenesis Of Ameloblastoma
The tumor may derive from the:
- Cell rest of enamel organ, either remnants of dental lamina or remnants of
- Hertwig’s Sheath, the epithelial rest cells of Malassez.
- Epithelium of odontogenic cyst.
- Disturbance of the developing enamel organ
- Basal cell of the surface epithelium of the jaw.
Histopathology Of Ameloblastoma
Histologically, the ameloblastoma shows neoplastic proliferation of odontogenic epithelial cells mostly in four distinct pattrns:
- Follicular type
- Plexiform type
- Acanthomatous type
- Granular type
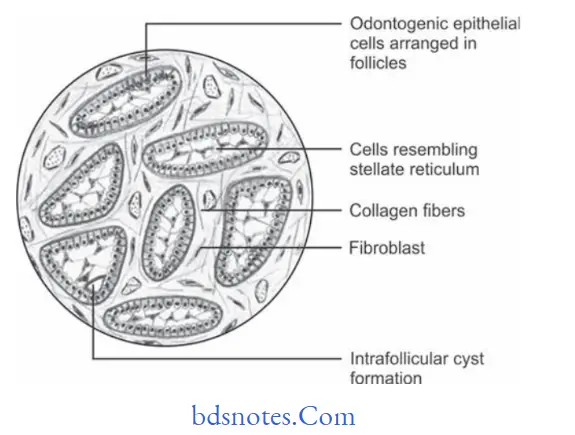
Follicular Type Of Ameloblastoma
“Steps to explain causes of odontogenic tumors: Genetic vs developmental factors: Q&A guide”
- Neoplastic odontogenic epithelial cells proliferate in form of multiple discrete follicles and islands within firous connective tissue stroma.
- Each follicle-like structure is bordered on the periphery by the single layer of tall columnar cells resembling ameloblasts-like cells.
Odontogenic Tumors Mcqs With Answers
- Cells located at the center of follicle are loosely arranged and resemble stellate reticulum cells.
- Microcyst formation is often observed inside these follicles.
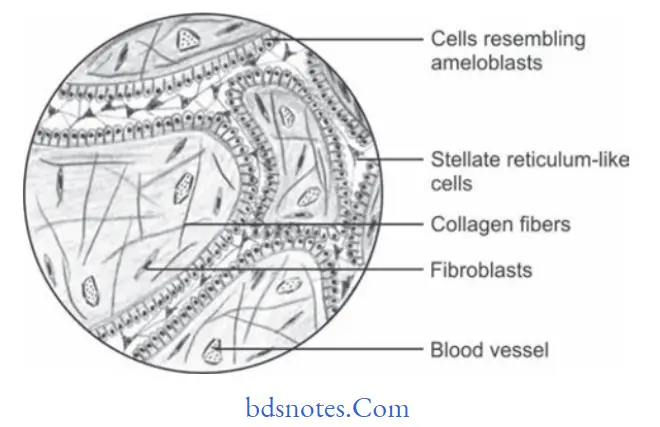
Plexiform Type Of Ameloblastoma
- Peripheral layer of cells are tall columnar in nature and often resemble ameloblast like cells.
- Cells situated at center portion of strands resemble stellate reticulum.
- Intervening connective tissue stroma is thin with minimum cellularity and shows multiple areas of cystifiation which may be either large or small in number.
“Role of dental lamina remnants in causing odontogenic tumors: Questions answered”
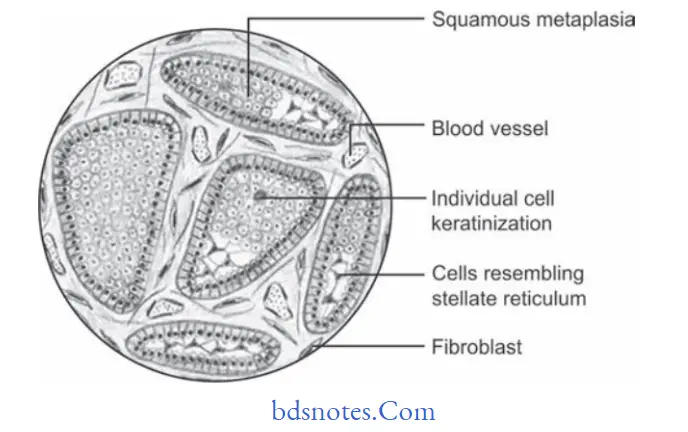
Acanthomatous Type Of Ameloblastoma
- Cells occupying the position of the stellate reticulum undergo squamous metaplasia, sometimes with keratin formation in the anterior portion of tumor islands.
- Occasionally, epithelial or keratin pearls may be observed.
Odontogenic Tumors Exam Questions
- Areas of calcification may be found in the metaplastic squamous epithelium.
- It may be confused with squamous cell carcinoma.
“How does abnormal tooth development lead to odontogenic tumors? FAQ explained”
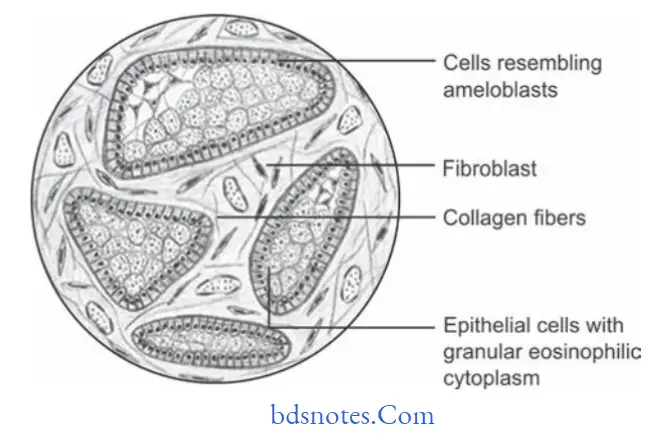
Granular Type Of Ameloblastoma
There is marked transformation of the cytoplasm, usually of the stellate reticulum like cells that it takes a very coarse granular eosinophilic appearance.
“Early warning signs of issues addressed by understanding odontogenic tumor pathogenesis: Common questions”
Clinical Features Of Ameloblastoma
- Ameloblastoma occurs in 2nd, 3rd, 4th and 5th decade of life.
- Mean age of occurrence is 32 years.
- Males are affcted more commonly than females.
- Ameloblastoma in most of the cases involves mandible in molar ramus area.
- Clinically ameloblastoma presents slow enlarging, painless, ovoid and fusiform bony hard swelling of the jaw.
- Pain, paresthesia and mobility of regional teeth is present in some cases.
- Pathological fractures may occur in many affcted bones.
Radiographical Appearance Of Ameloblastoma
- During the early stage area of bone destruction is well defied and have hyperostotic borders.
- Outline of margins of lesion is smooth, well defied, scalloped and is corticated.
- Ameloblastomas are mostly multilocular but at times they are unilocular too.
- It reveals honeycomb appearance because of arrangement of septae. It also reveal soap bubble appearance if larger compartments are present.
Odontogenic Tumors Viva Questions
- Presence of bony expansion and thinning of cortical plates which leaves thin egg shell of bone which is known as egg shell crackling.
- Extensive root resorption is seen in lesional area.
Treatment Of Ameloblastoma
- Patients with conventional solid or multicystic intraosseous ameloblastoma are treated by simple enucleation to curettge to en bloc resection.
- Marginal resection is the most widely used treatment. But recurrence rate up to 15% are evident.
- Some surgeons adopt conservative approach by planning surgery after careful CT scan evaluation. Removal of tumor is done followed by peripheral ostectomy.
- Other surgeons advocate that margin of resection should be 1 to 1.5 cm past radiographic limits of tumor.
“Asymptomatic vs symptomatic effects of ignoring odontogenic tumor causes: Q&A”
Question 2. Write short note on adenomatoid odontogenic tumor.
Answer. Adenomatoid Odontogenic Tumor
It is also called adenoameloblastoma or ameloblastic adenomatoid tumor.
Adenomatoid odontogenic tumor is uncommon, well-circumscribed, odontogenic neoplasm characterized by the formation of multiple duct-like structures by neoplastic epithelial cells.
Clinical Features Of Adenomatoid Odontogenic Tumor
- Tumor usually occurs in younger age.
- Females are more commonly affected
- Lesion most typically appears in maxillary anterior region.
- Tumor presents a slow enlarging, small, bony hard swelling in maxillary anterior region.
- Sometimes, it occurs in premolar region
- There is displacement of regional teeth, mild pain and expansion of cortical bones.
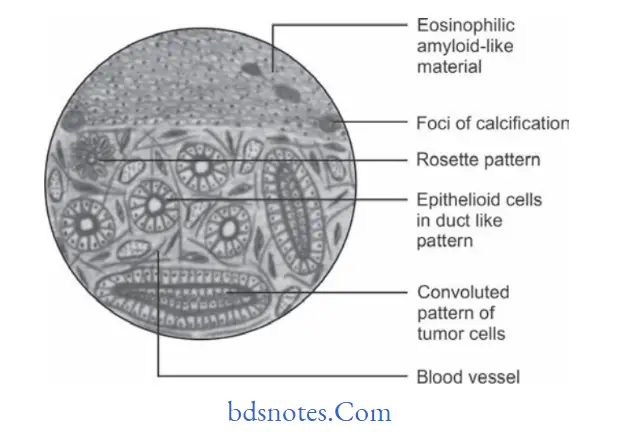
Histopathology Of Adenomatoid Odontogenic Tumor
- Microscopically, adenoid odontogenic tumor reveals neoplastic odontogenic epithelial cells, proliferating in multiple “duct like” pattrns.
- Presence of these duct like structures often give glandular lesion.
- Each duct like structure is bordered on periphery by a single layer of tall columnar cells resembles ameloblastoma.
Odontogenic Tumors Quiz Questions
- Lumen of duct-like structures are filled with the homogenous eosinophilic coagulum.
- Small foci of calcifications are often seen, which are scattred throughout the lesion.
- Droplets of amorphous (PAS positive) eosinophilic material are found between neoplastic cells.
“Can targeted interventions improve outcomes using knowledge of odontogenic tumor etiology? Answer provided”
Differential Diagnosis Of Adenomatoid Odontogenic Tumor
- Dentigerous cyst
- Odontomes
- Unicystic ameloblastoma
- CEOT
- CEOC.
Treatment Adenomatoid Odontogenic Tumor
The treatment is surgical enucleation.
Question.3. Write short note on Pindborg tumor.
Or
Describe in brief Pindborg tumor.
Or
Write short note on CEOT.
Answer. Pindborg tumor is locally aggressive neoplasm, which is also known as calcifying epithelial odontogenic tumor.
Pathogenesis Of Pindborg tumor
- Some investigators suggest that the Pindborg tumor arises from remnants of cells in stratum intermedium layer of the enamel organ in tooth development. Some hypothesize that the Pindborg’s tumor arises from the remnants of the primitive dental lamina.
- Definite etiology of neoplasm still remains enigmatic.
Clinical Features Of Pindborg tumor
- Tumor occur in middle age persons.
- Mandible is involved more often than maxilla.
- Molar region is more common site of occurrence followed by premolar region.
- Tumor presents a slow enlarging, painless swelling of jaw with expansion and distortion of cortical plates.
- Swelling is bony hard and clinically, it is well defined or diffused.
- Pain, paresthesia may develop on rare occasions and few lesions may be completely asymptomatic.
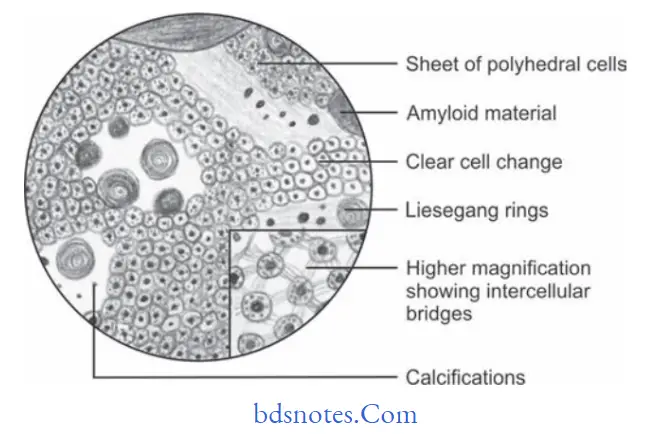
Histopathology Of Pindborg tumor
- Tumor reveals sheet of closely packed, polyhedral cells in noninflmed connective tissue stroma.
- Tumor cells contain ovalshaped nuclei and homogenous eosinophilic cytoplasm.
- Prominent intra cellular bridges and distinct cell boundaries are often found in the lesions.
- Some amount of homogenous, hyaline material is often deposited in between tumor cells called amyloid material.
- One of the most important histological characteristics of CEOT is the presence of several calcifid masses in and around the tumor cells.
- Some Liesegang rings are also found.
“Differential applications of benign vs malignant odontogenic tumors: Questions answered”
Treatment Of Pindborg tumor
Surgical enucleation is done.
Odontogenic Tumors Mcqs With Answers
Question.4. Write note on odontoma.
Or
Write short note on odontome.
Answer. Odontomas are hamartoma that contain both epithelial and mesenchymal dental tissue components.
- Generally, there are two types of odontoma:
1. Complex odontoma
2. Compound odontoma.
Complex Odontoma
It is always benign and contains enamel, dentin and cementum which are not differentiated, so that structure of actual tooth is not identifible.
Compound Odontoma
It is also benign. In compound odontomas, the enamel and dentin are laid down in such a fashion that the structure bears considerable anatomic resemblance to normal teeth, except that they are often smaller than typical teeth.
Clinical Features Of Odontoma
- Lesion occurs among children or young adults.
- Both sexes are equally affected or slight male predominance is present.
- Maxilla is commonly affected. Odontomas are commonly seen in pericoronal area of permanent teeth.
- Odontoma produces large, bony, hard swellings of jaw, with expansion of cortical plates and displacement of regional teeth.
Odontogenic Tumors Exam Questions
- If odontoma is located high in alveolus, they may tend to erupt in oral cavity by resorbing overlying bone and as a result there may be pain, inflammation, ulceration, etc.
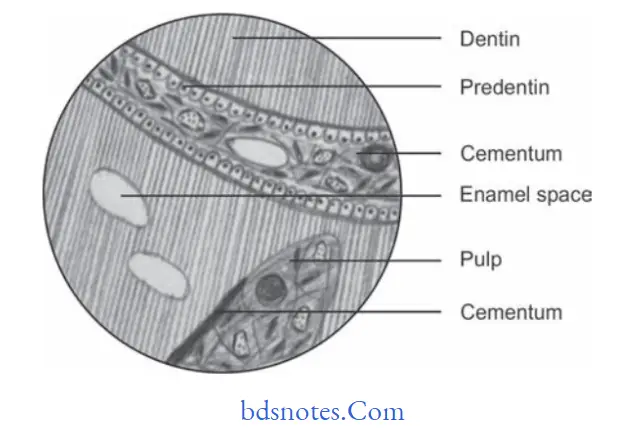
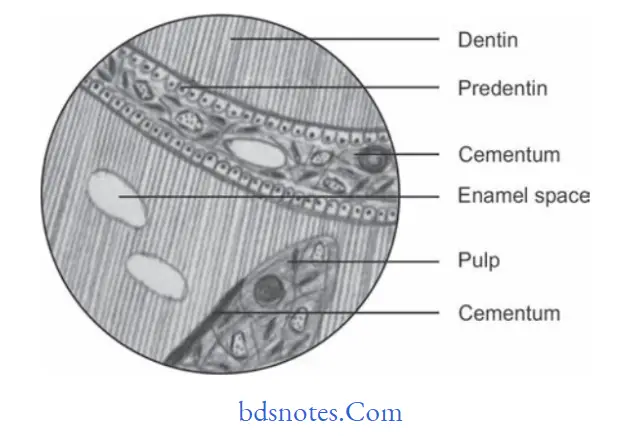
Histopathology Of Odontoma
“Steps to educate patients about odontogenic tumors and their importance: Q&A format”
- Fully developed compound odontoma reveals the presence of encapsulated mass of separate denticles, embedded in firous tissue stroma.
- The fully developed complex odontoma reveals an irregularly arranged but wellformed mass of enamel, dentin and cementum which is surrounded by firous tissue capsule.
- The dentinal tissues lie in the direct contact with connective tissue that resembles the dental pulp.
- Most of enamel tissues are fully calcified and appear as small empty space.
“Role of counseling in clarifying goals for managing odontogenic tumors: Questions answered”
Treatment Of Odontoma
Surgical Enucleation.
Odontogenic Tumors Viva Questions
Question.5. Write short note on histopathological variants of ameloblastoma.
Or
Write in detail on histopathological types/variants of ameloblastoma.
Answer. Following are the histopathological variants of ameloblastoma
- Desmoplastic type: There is the presence of marked hyalinization of connective tissue stroma.
- Basal cell type: Tumor islands show basaloid pattrn of cells.
- Clear cell type: Solid multicystic ameloblastoma may contain clear cells which are localized to the stellate reticulum-like areas of follicular ameloblastoma.
- Keratoameloblastoma and papilliferous keratoameloblastoma:
- Ameloblastoma consists partly of keratinizing cysts and partly of tumor islands with papilliferous arrangement
- Mucous cell differentiation type: Follicular ameloblastoma showing focal mucous cell differentiation.
- Hemangiomatous ameloblastoma: It is an ameloblastoma in which part of the tumor contain spaces filed with blood or large endothelial-lined capillaries.
Malignant odontogenic tumors
Odontogenic Tumors Question Bank
“How do educational materials explain complex odontogenic tumor concepts? FAQ explained”
Question.6.Classify odontogenic tumors. Describe in detail etiopathogenesis, clinical features, radiology, histopathologic features, and differential diagnosis of adenomatoid odontogenic tumor.
Or
Give classification of odontogenic tumors. Discuss about clinical features and histopathology of AOT.
Or
Classify odontogenic tumors. Write in detail about adenomatoid odontogenic tumors.
Answer.
Etiopathogenesis Of Odontogenic Tumors
- Since adenomatoid odontogenic tumor occurs within toothbearing areas of ja, it arises from reduced enamel epithelium during the presecretory phase of enamel organ development.
- Some category of authors also believes that it arises from dental lamina or from preexisting dentigerous cyst.
Radiology Of Odontogenic Tumors
- Radiographically tumor presents a wellcircumscribed unilocular radiolucent area which consisted of impacted tooth or odontome and exhibits a smooth corticated border.
- Multilocular radiolucencies are also seen rarely with scalloped borders.
- At times radioopaque foci is detectable within radiolucent lesion.
- As lesion progresses divergence of roots and displacement of teeth is seen.
“Early warning signs of knowledge gaps in patient understanding of odontogenic tumors: Common questions”
Question.6.Classify odontogenic tumors. Write in detail about the clinical, radiological, and histological features of calcifying epithelial odontogenic tumor.
Answer.
Radiological Features Of Odontogenic Tumors
- Radiographically tumor consists of either a unilocular or multilocular radiolucent defect with radiolucent to radiopaque area surrounding the crown of impacted tooth.
- Radiopacity is of proteinaceous material released by the tumor cells. The radiopaque structures are of varying size and density and are scattered all over which provides the lesion a driven snow appearance
- Margins of the lesion are scalloped and are well defied.
- Tumor can displace the developing tooth.
- Cortical plate expansion is also appreciated buccally, lingually, and in vertical dimensions.
Leave a Reply