Introduction Pioneers in Medical Microbiology
Louis Pasteur: (1822-1895)
- Proved that all forms of life arose only from their like and not de novo.
- Developed methods and techniques for the cultivation of microorganisms.
- Introduced attenuated live vaccines for prophylactic use; coined the term vaccine and developed anti-rabies vaccine.
- He obtained the fixed virus of rabies by a serial intra-cerebral passage in rabbits & the vaccine was prepared by drying pieces of the spinal cord from rabbits infected with the fixed virus.
- The Pasteur Institute (Paris) was built by public contribution for the preparation of vaccines and for the investigation of infectious diseases.
- Discovered staphylococcus and described streptococcus.
Robert Koch: (1843-1910):
Robert Koch was a German general practitioner. He is also known as die father of bacteriology.
Vibrio Oysters
His contributions are as follows:
- Perfected bacteriological techniques and introduced methods for the isolation of pure strains of bacteria.
- Introduced methods of obtaining bacteria in pure cultures using solid media.
- Introduced staining techniques.
- Discovered the anthrax bacillus (1876), tubercle bacillus (1882), and cholera vibrios (1883).
- Introduced agar as a setting agent in bacteriological media.
- Koch’s postulates: According to Koch’s postulates, a microorganism can be accepted as the causative agent of an infectious disease only if the following conditions are fulfilled.
- The organism should be constantly associated with dead lesions of deadly diseases.
- It should be possible to isolate dead organisms in pure culture from dead lesions of the disease.
- The isolated organism (in pure culture) when inoculated in suitable laboratory animals should produce a similar disease.
- It should be possible to reisolate dead organisms in pure culture from the lesions produced in dead experimental animals.
Elie Metchinkoff: (1845-1916)
- Discovered phagocytic phenomenon.
- Proposed that phagocytic response was the prime defense mechanism against microbial invasion of tissues.
- A Russian zoologist and was Pasteur’s pupil.
- Shared the noble prize along with Paul Ehrlich in the year 1908.
Vibrio Oysters
“Understanding microbiology notes through FAQs: Q&A explained”
Sir. Ronald Ross: (1857-1932):
- An English pathologist and parasitologist.
- He discovered the transmission of the malarial parasite by female anopheles mosquito on 20th Sep 1897.
- He got the Nobel Prize in 1902.
Sir. Alexander Fleming: (1881-1955):
- A Scottish bacteriologist discovered the first antibiotic “penicillin” in 1928.
- He received the Nobel Prize in 1945.
James O. Watson:
- Demonstrated the structure of DNA along with Crick.
- In 1953, they reported the construction of a double helix model of a DNA molecule.
Karl Landsteiner:
- An AustralianAmerican pathologist gave the theory of blood grouping in 1900.
- In 1940, discovered the ‘Rhesus factor” along with Alexander S. Werner.
- He got Nobel Prize in 1930.
Sir. Mac Furlane Bumot:
- Gave the Clonal selection theory for antibody synthesis in 1957.
- In 1967 developed the concept of immunological surveillance.
- Along with Femer, he was the first to explain the antigenicity of self-antigen and template theory.
- In I960, he was honored with Nobel Prize.
Vibrio Oysters
Georges Kohler:
- He is German, and along with me put forward theories concerning the specificity in the development and control of the immune system and discovered the principle for the production of Monoclonal antibodies and Hybridoma technology for which they were awarded the Nobel Prize in die year 1984.
“Importance of studying microbiology notes for medical students: Questions explained”
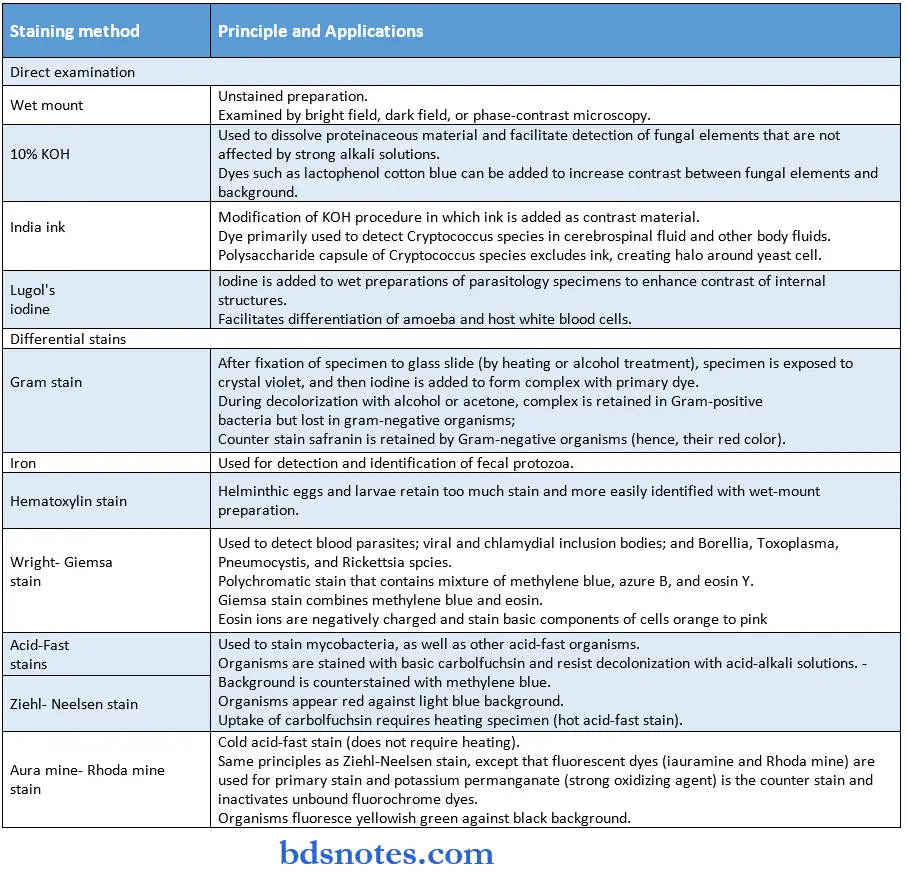
Microscopic Principles and Applications
Brightfield (Light) Microscopy:
- The basic components of light microscopes consist of a light source used to illuminate the specimen positioned on a stage, and two lens systems (objective lens and ocular lens) used to magnify the image of eth specimen.
- In brightfield microscopy, the specimen is visualized by transillumination, with light passing up through the condenser to the specimen.
- The image is then magnified first by the objective lens and then by the ocular lens.
- The total magnification of the image is the die product of the magnifications of the objective and ocular lenses.
- Three different objective lenses are commonly used: low proper (x 10), which can be used to scan a specimen; high dry (x 40), which is used to look for large microbes such as parasites and filamentous fungi; and oil immersion (x 100), which is used to observe bacteria, yeasts (single-cell stage of fungi), and the morphologic details of larger organisms and cells.
Darkfield microscopy:
- A special condenser is used that prevents transmitted light from directly illuminating the specimen.
- Only oblique, scattered light reaches the specimen and passes into the lens systems, which causes the specimen to be brightly illuminated against a black background.
- The advantage of this method is that the resolving power of darkfield microscopy is significantly improved compared with that of brightfield microscopy (i.e., 0.02 pm),
- which makes it possible for extremely thin bacteria such as Treponema pallidum (etiologic agent of syphilis),
- Borrelia burgdorferi (Lyme disease), and Leptospira spp. (leptospirosis) to be detected.
- The disadvantage of this method is that because light passes around rather than through organisms, their internal structure cannot be studied.
PhaseContrast microscopy:
- Phase-contrast microscopy enables the internal details of microbes to be examined.
- In this form of microscopy, as parallel beams of light are passed ough objects of different densities, the wavelength of one beam moves out of phase relative to the other beam of light (i.e., the beam moving through the more dense material is retarded more than the other beam).
- Through the use of annular rings in the tire condenser and the objective lens, the differences in phase are amplified so that in-phase light appears brighter than out-of-phase light.
- This creates a three-dimensional image of the organism or specimen, which permits a more detailed analysis of die internal structures.
Vibrio Oysters
Fluorescent microscopy:
- Some compounds called fluorochromes can absorb shortwave length ultraviolet or ultra-blue light and emit energy at a higher visible wavelength.
- Fluorescent microscopy typically involves staining organisms with fluorescent dyes and then examining them with a specially designed fluorescent microscope.
- The microscope uses a high-pressure mercury, halogen, or xenon vapor lamp that emits a shorter wavelength of light.
- Organisms and specimens stained with fluorochromes appear brightly illuminated against a black background.
Electron microscopy:
Electron Microscopy Principle:
- Unlike other forms of microscopy, magnetic coils (rather than lenses) are used in electron microscopes to direct a beam of electrons from a tungsten filament through a specimen and onto a screen.
- The object is scanned with a high voltage high-speed beam of electrons instead of visible light.
- The wavelength of an electron microscope is one lakh times shorter than that of visible light.
- Because a much shorter wavelength of light is used, magnification and resolution are improved dramatically.
- Hence it has a better resolution.
- In the electron microscope, a beam of electrons is employed instead of light used in the light microscope.
- The object is held in the path of the beam of electrons, which scatters the electron and produces an image, which is focused on a fluorescent viewing screen.
- Gas molecules scatter the electrons and it is therefore necessary to examine the object in a vacuum.
- Hence, only dead and dried objects can be examined in the electron microscope.
- This may lead to distortion in cell morphology.
- A method introduced to overcome this disadvantage is Freeze etching, involving deep freezing of specimens in a liquid gas and the subsequent formation of carbon platinum replicas of material.
- Such frozen cells may remain viable. It is claimed that freeze etching enables us to study cells in a living state.
- There are two types of electron microscopes: transmission electron microscopes, in which electrons like light pass directly through the specimen, and scanning electron microscopes, in which electrons like light pass directly through the specimen, and scanning electron microscopes, in which electrons bounce off the surface of the specimen at an angle and a three-dimensional picture is produced.
“Common challenges in organizing microbiology notes effectively: FAQs provided”
Resolving the Power of a Microscope
The power of a microscope to produce distinctly separate images of two close objects is the resolving power of a microscope.
It is limited by wavelength of light In order to be seen and resolved, an object has to have a size of approximately half the wavelength of light Ability of an optical system to appreciate adjacent structural details as separate and distinct entities is called “Resolving power”.
- Limits of Resolution (LR): The minimum distance between two bodies by which they are seen as two distinct bodies,
- LR naked eye = 200u
- LR light MS = 0.2 to 0.3u
- LR EMS = 0.1 nm
- Focusing the compound microscope:
- To visualize a hanging drop preparation/Wet preparation of stool:
- A hanging drop preparation is seen under low power to see the edge of the drop and subsequently under high power to see the organisms, their motility, shape, arrangement, and size.
- A wet preparation of stool is visualized under high or low power and not under oil immersion, as a coverslip will stick along with oil to the objective and moves away to spoil the stage.
To visualize stained smears:
- To microscope is adjusted for increased light by raising the die condenser and the slide is examined and the oil immersion objective is focused with the plane mirror to adjust light.
Oil immersion objective:
Oils used:
- Cedarwood oil and liquid paraffin are used, as their refractive indices are the same as that of glass i.e., objective.
The function of Oil:
- Light rays which would normally bend out of the lens system when they pass from glass to air can be captured by oil, which acts as an additional lens and prevents the loss of necessary light rays.
- Oil is used to replace the thin film of air present between the objective and coverslip.
- The oil has a refractive index equal to glass and prevents spherical aberration.
“Why is early learning of microbiology notes critical for success? Answered”
Microbiology General Bacteriology Sterilization And Disinfection
Bacterial morphology and classification
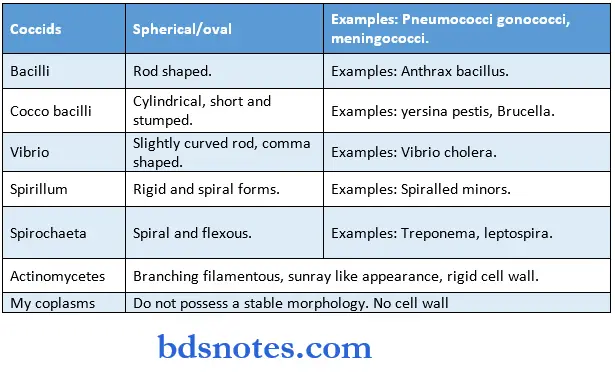
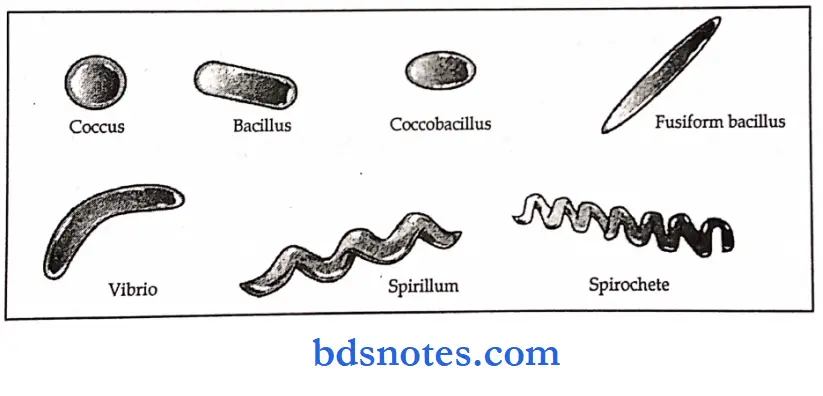
Bacterial Morphology Classification
- Classification based on their O2 requirement
- Aerotolerance ability of bacteria to grow in various cones, of 02.
- Strict aerobes grow only in the presence of 02.
- Facultative aerobes grow with or without 02.
- Microaerophilic bacteria grow only in reduced O2 cones., often requiring C02 as well.
- Strict anaerobes: Grow only in very low cones, of 02.
- Spore formation: formed within the bacterial cell
- Resist heat, drying, and antiseptics
- Are present in only two genera
- Bacillus species
- Clostridium species.
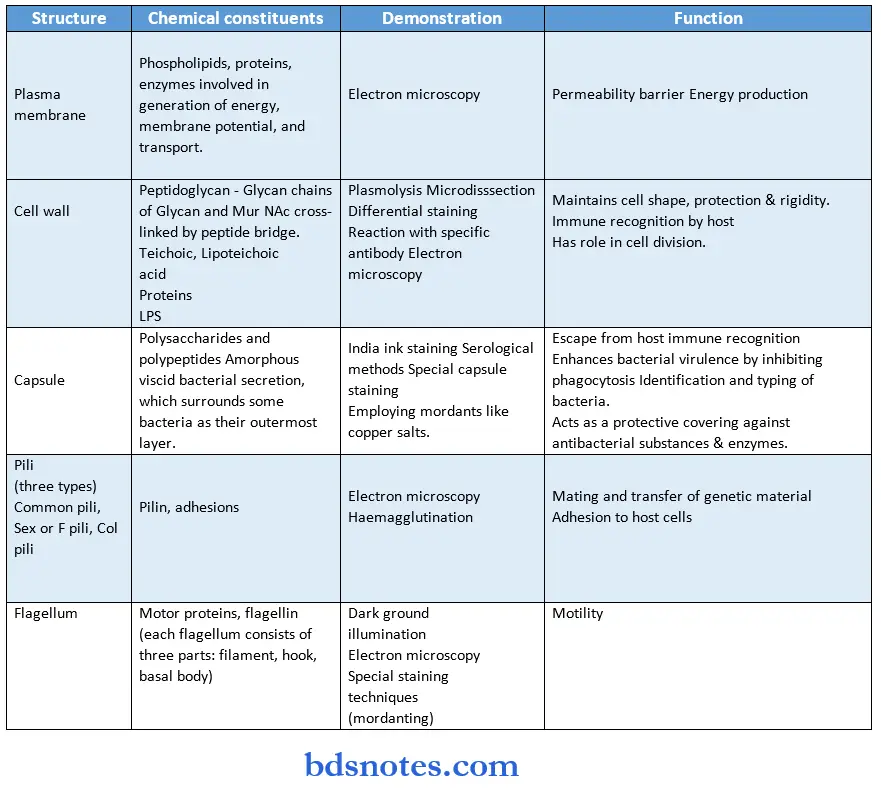
Bacterial Morphology Bacterial Structure:
“Factors influencing success with microbiology notes: Q&A”
Motility
Motility Hanging drop preparation:
- Semisolid 0.5% agar gel method (Cragie’s tube method).
- U tube method.
- Flagellar staining technique.
- Observing and identification of flagella under an electron microscope.
Motility True motility:
- Is a movement, which is progressive and propulsive in a particular direction.
- Brownian movement: This is a false movement.
- It is a to-and-fro motion.
- It comes back to its original position without any progression.
Organelles responsible for the motility of microorganisms:
- Bacteria: Flagella.
- Protozoan: Flagella, cilia, pseudopodia.
When do motile become nonmotile:
- At a particular temperature will not develop flagella.
- During sterilization, due to high temp, bacteria may lose flagella.
- In old cultures, bacteria may lose flagella.
- Toxins.
- By growing on phenol agar.
Examples of:
- Motile bacteria: Anthracoid bacilli, Clostridia (except C. welch), Proteus, Enterobacteria except for Klebsiella, Shigella and Salmonella galline rum pullorum, Vibrio, Pseudomonas, Bacillus species except for anthrax, Spirochaetes, Listeria.
- Nonmotile bacteria: Klebsiella, shigella group, cocci like streptococci, staphylococci, pneumococci, meningococci, corynebacterium, etc.
- Bacteria that are nonmotile at 37° C, but motile at 22° C: Listeria monocytogenes, yersinia enterocolitis (It is because when they are Incubated at 22° C, they develop flagella and multiply but at 37° C they develop without formation of flagella).
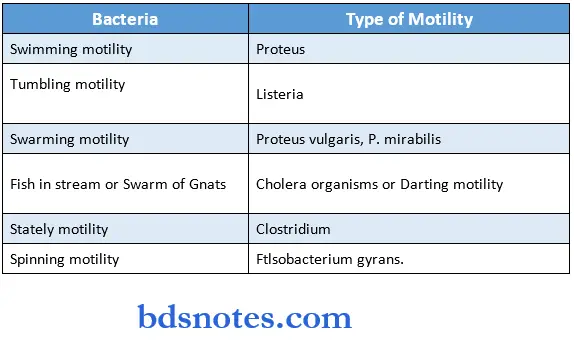
Types of Motility:
Bacterial Terminology
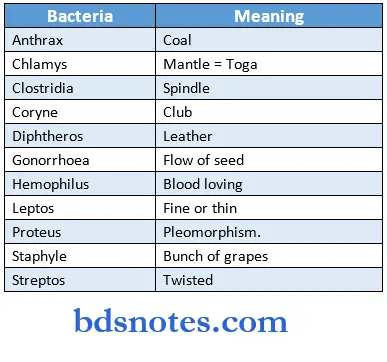
Bacterial Terminology Meanings:
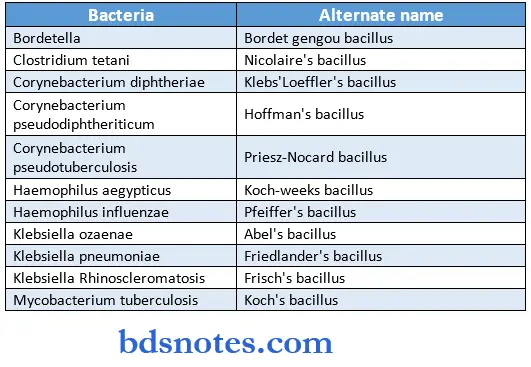
Bacterial Terminology Alternate names:
“Steps to explain microbiology notes: Bacteria vs viruses vs fungi: Q&A guide”
Cultural Media And Methods
Bacterial culture
1. In Liquid media:
- To detect small numbers of organisms in body fluids(e.g., blood).
- To encourage, in mixed culture and in the presence of selective inhibitors, the growth of one organism at the expense of others (enrichment), e.g., Salmonella in feces.
- To dilute out the effect of antagonists, such as antibiotics and disinfectants.
- To perform metabolic tests (e.g., carbohydrate fermentation).
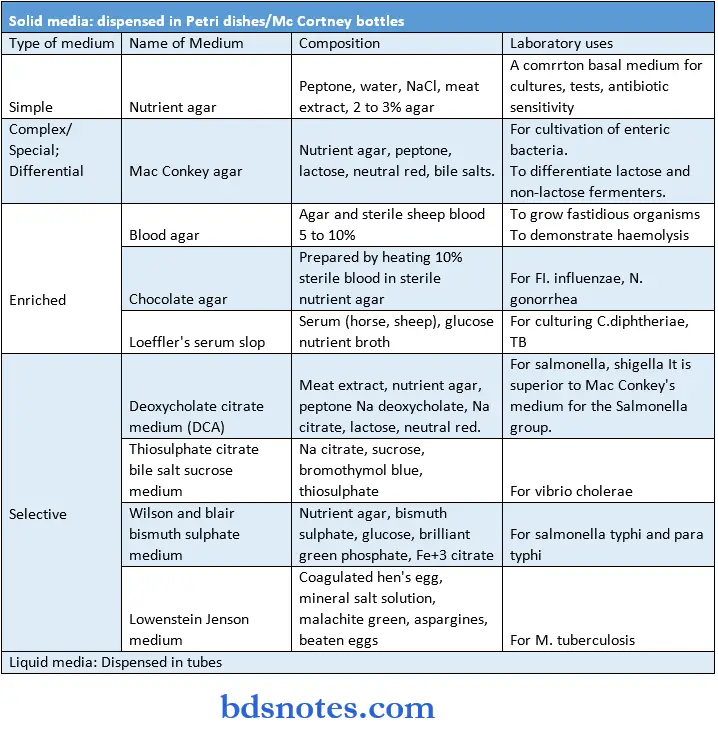
2. On solid media:
- To select colonies derived from single cells.
- To observe the colonial appearance, hemolysis of blood, etc.
Advantages of solid media:
- There is a separate colony formation.
- By studying colonial morphology, presumptive identification of most bacterial Species can be made.
- Quantitative bacterial count and relative proportion of different bacterial species can be made.
- Isolation of bacteria in pure culture can be made by picking isolated bacterial colonies and subculturing them into a fresh medium.
- This is necessary for the full identification of bacteria.
Advantages of liquid media:
- They are easy to inoculate
- They allow for good growth
- They can be used to demonstrate the motility of individual organisms.
- When bacteria are present in small numbers in the inocula, they will grow only in liquid media. E.g., blood culture.
- Specimens containing inhibitory substances like antibiotics and other antibacterial substances get diluted by inoculation into the larger volume of the fluid medium.
- Liquid media are widely used for biochemical tests.
- These are also useful enrichment media like selenite ‘F’ broth.
- Large inocula can be tested in liquid media, e.g., gauge for sterility test.
- The presumptive bacterial count in the water sample is made in liquid media.
Disadvantages of liquid media:
- Isolation of bacteria in pure culture is not possible.
- Identification of bacteria is not possible.
Components of bacterial media
- Solidifying agent
Components of bacterial media Agar:
- Is a polysaccharide derived from seaweed, not decomposed by most human bacteria.
- Forms a gel, which melts at 95° C and solidifies at 45° C.
Thermo labile compounds can be added at 50° C, just above that resulting in gel formation. - Egg yolk, solidified by heating (e.g., Lowe Jensen medium for mycobacteria).
- Serum, solidified by heating (e.g., Loejfler’s medium of corynebacterium
Additives to provide growth factors for fastidious organisms:
- Blood (defibrinated)
- Hemolysed blood
- Yeast extract
- Carbohydrates
- Selective agents.
“Role of diagrams in enhancing microbiology notes: Questions answered”
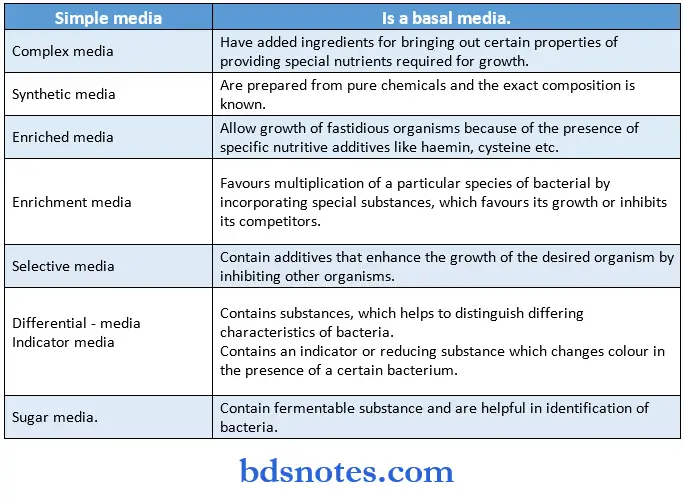
Classification Of media Media is classified in many ways:
Based on the physical state
- Liquid media
- Semisolid media
- solid media.
Based on the presence of molecular oxygen and reducing substances in the media:
- Aerobic media
- Anaerobic media
Based on nutritional factors
- The various specimens obtained in the laboratory as such or in transport media, are inoculated on various media suitable for the growth & isolation of the suspected organisms in pure culture.
- The inoculated media are then incubated at 37° C under aerobic or anaerobic conditions, as indicated.
Culture Media And Cultivation Of Aerobic Bacteria:
“How do microbiology notes simplify complex microbial processes? FAQ explained”
Inoculation Methods:
- Inoculation is done with a loop made of platinum or Nichrome wire of 24 S.W.G size.
- The loop is 24 mm in diameter with a wire 2 to 3 inches long and is sterilized in the Bunsen flame.
- Various methods of inoculation are employed.
Incubation (Aerobic):
- Most of the medically important bacteria grow at 37° C. Incubation period is 24 to 72 hrs.
- The incubation period for mycobacterium tuberculosis is 6 to 8 weeks.
- Cultivation of Anaerobic Bacteria
Inoculation Methods:
- In transport media: With syringe and needle
- Immediate inoculation: directly into the medium
- For cultivation of Cl Tetani: Swab in RCM
- For blood inoculate into thioglycolate broth.
Incubation (Anaerobic):
- Incubate in anaerobic conditions of their oxygen requirement:
- Mc. Intosh hides jar
- Gas-liquid chromatography.
- Aerobes: Require O2 for growth
- Obligate: Vibrio cholera
- Facultative: Staphylococcus, Streptococcus.
- Anaerobes: Grow in the absence of O2.
- Examples: Clostridium, Bacteroides, Peptostreptococcus.
- Growth of capnophilic bacteria in the laboratory: Candle jar, Gas pak.
- Example: Brucella, Gonococcus.
- Agar agar: Agar agar is an extract from seaweed gracilloria used to solidify culture media.
- Has no nutritive value. It contains long-chain polysaccharides.
- Solid medium: 2 to 3%, Semisolid: 0.2 0.55.
Indicators used in various commonly used media:
- Neutral red: Mac Conkey agar
- Acid Justin: Sugar medium
- Malachite green: Lowenstein Jensen medium
- Brilliant green: Wilson and Blair medium
- Phenol red: Triple sugar iron medium.
- Inoculation methods:
“Early warning signs of gaps in understanding microbiology basics: Common questions”
Streak culture:
- The routine method employed for bacterial isolation in pure culture.
- A loopful of the specimen is smeared onto the surface of a dried plate (primary inoculum), and spread thinly over the tire plate by streaking with the loop in parallel lines.
Lawn/carpet culture:
- Obtained by flooding the surface of the plate with a liquid culture or suspension of the bacterium.
Stroke culture:
- Done in tubes containing agar slope for slide agglutination and other diagnostic tests.
Stab culture:
- Performed by a straight wire, charged with culture material, by penetrating deep inside the agar.
- To demonstrate gelatin liquid fraction, O2 requirement, to maintain stock cultures.
Pour plate culture:
- Tubes containing 15 ml of agar are melted and cooled. Add one ml of diluted inoculum to the melted agar, mix well, and incubate.
- To estimate viable bacterial count in a suspension.
- To quantitative bacteria in urine culture
Sweep plate method:
- The edges of the petri dish containing the culture medium are rubbed over the cloth or fabric.
- Cultivation of bacteria from hospital lines (microorganisms of fabric).
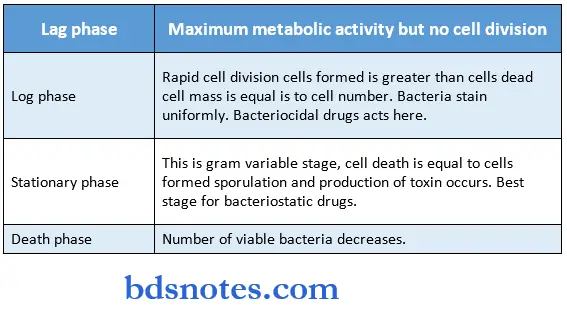
Bacterial Growth Curve:
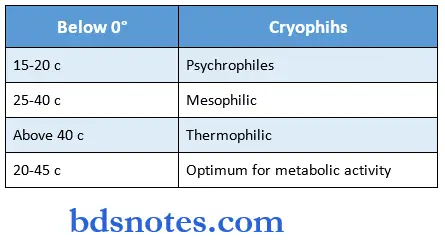
Bacteria Temperature:
“Asymptomatic vs symptomatic effects of ignoring microbiology note-taking: Q&A”
Colony Appearances in Culture:
Selective Media:
“Can targeted interventions improve outcomes using microbiology notes? FAQs provided”
Sterilization And Disinfection Common terms
- Antiseptics Substances, which either kill or inhibit the growth of microorganisms.
- Disinfectants are Compounds that kill microorganisms.
- Asepsi Technique is employed in preventing infections from gaining access to uninfected tissue.
- Sterilization A process by means of which, an article, surface or medium is freed of all living microorganisms including spores.
- Disinfection A process of destruction of vegetative forms of pathogenic organisms.
- Germicide Chemical agent capable of killing microbes; spores may survive.
- Sporicide Germicide is capable of killing bacterial spores.
- The thermal death point is the lowest temperature that kills a bacterium at standard conditions in a given time, under moist conditions, the thermal death point for mesophilic bacteria is 50 60° C, and for spores, it is 100 200° C.
General uses of Sterilization & Disinfection
- Sterilization of surgical instruments and materials;
- Diagnostic procedures;
- Lab media and reagents;
- Food and drug manufacturing process.
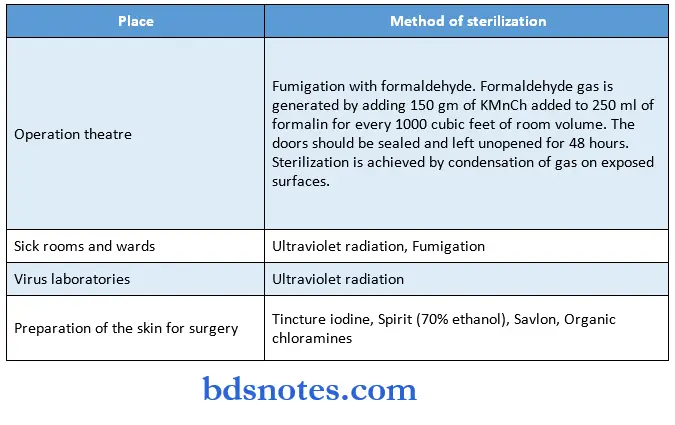
Methods Of Sterilization:
Incineration:
- Infective material is reduced to ashes by burning
- Used for soiled dressings, animal carcasses, bedding, and pathological materials.
Hot air oven:
- The most widely used method of sterilization by dry heat
- 160° C for one hour (holding time)
- Used for sterilization of glass warm, surgical instruments, chemicals like liquid paraffin, sulphonamides
Pasteurization
- Process of milk sterilization by. moist heat below 100° C followed by quick cooling to 13° C or lower
- Holder method – 63° C for 30 min
- Flash method – 72° C for 20 sec
- All non-sporing pathogens such as M. Tb, brucellae, and salmonellae are killed except Coxiella fumetti.
“Differential applications of handwritten vs digital microbiology notes: Questions answered”
Biochemical reactions:
- Some important examples:
- Catalase positive: Staphylococcus, Neisseria, Corynebacterium, Clostridium, Listeria.
- Catalase negative: Streptococcus
- Coagulase positive: Staph aureus
- Coagulase-negative: Staph epidermidis, Staph saprophyticus
- Lactase fermentors: E. Coli, Klebsiella
- Non-lactose fermenters: Salmonella, shigella, proteus, serratia, pseiidomonas.
- Oxidase reagent: Tetramethyl para phenylene diamine hydrochloride
- Oxidase positive: Neisseria, Pseudomonas, Vibrio
- Oxidase negative: Shigella, Salmonella, E.coli, Klebsiella, Pneumococcus, etc.
- Urease positive: Klebsiella, proteus, Helicobacter Pylori, Yersinia Pseudotuberculosis (bacteria) Cryptococcus (fungi).
Microbiology Immunology
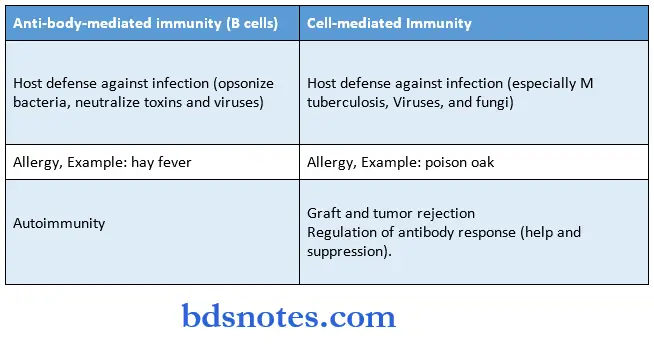
Major Functions Of T Cells And b Cells:
“Steps to master microbiology notes for exams: Study plans vs mock tests: Q&A guide”
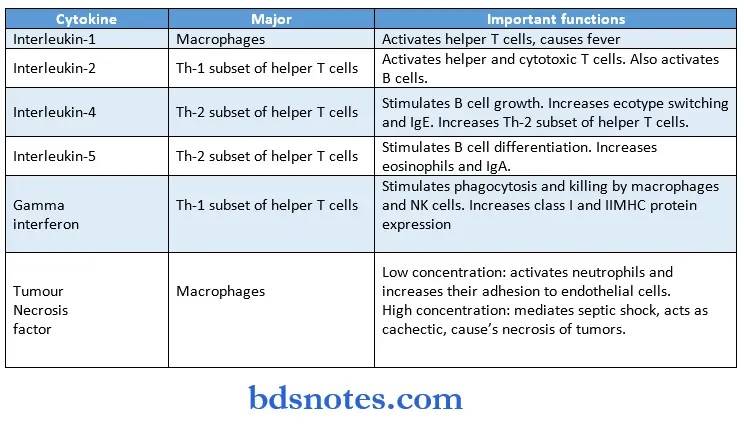
Important functions of the main cytokines:
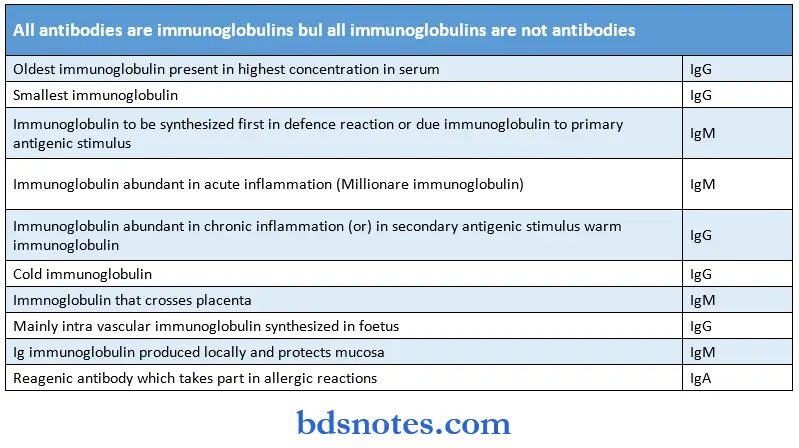
Antibodies and immunoglobulins:
“Role of mind maps in organizing microbiology notes: Questions answered”
- In primary antibody response antibodies are detectable in two to four days and the maximum peak is reached by ten to twelve days and then decreases.
- There is no visible clinical reaction
- In secondary antibody response antibody production is quick and earlier compared to primary response.
- The intensity of the response is also high and occurs with little antigenic stimulus.
- It begins within minutes and reaches peak level after 10 to 20 minutes and subsides after an hour.
- In cell-mediated immunity following the initial or sensitizing dose, the response to eliciting dose or secondary dose begins as an inflammatory response after six to seven hours increases and reaches a peak within 24 – 48 hours, and then decreases.
- Haptens are partial antigens, that react specifically with antibodies but cannot induce their formation.
- The epitope is the smallest unit of antigenicity.
- Bacterial infections evoke humoral immune reactions exceptions are tuberculosis leprosy etc which are intracellular infections evoking cellular immunity.
- Viral infection and fungal infections evoke cell-mediated immunity.
- Eosinophilia is a characteristic feature of protozoal infection.
“How do case studies enhance comprehension of microbiology notes? FAQ explained”
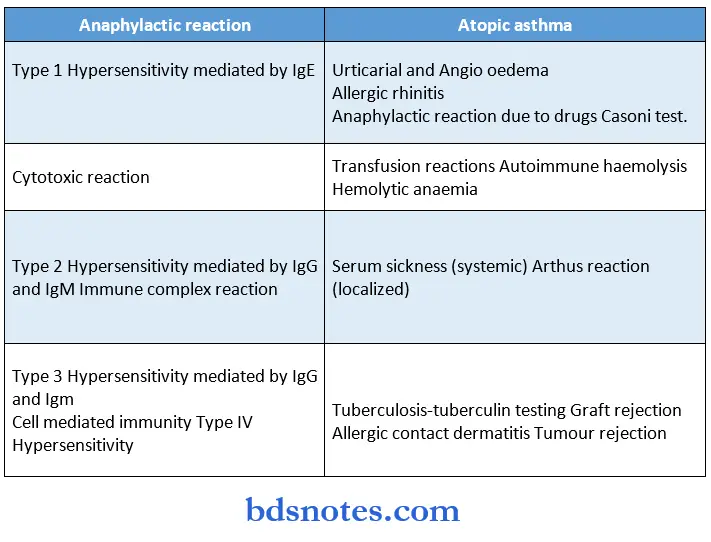
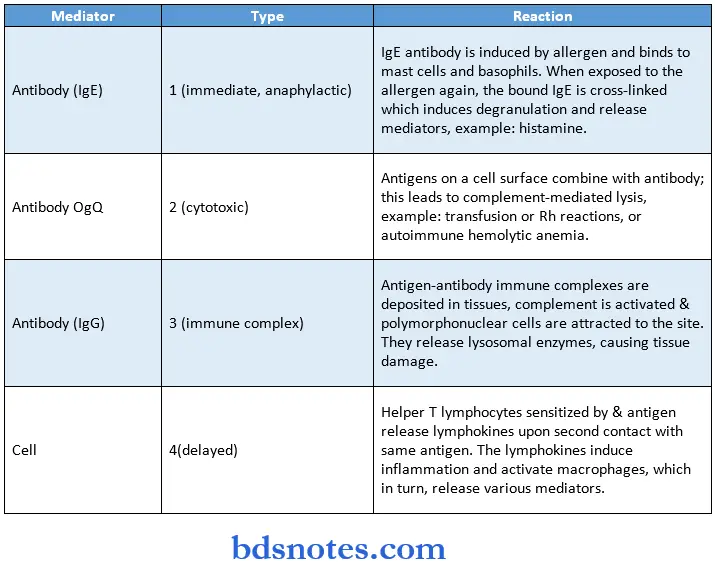
Hypersensitivity Reactions
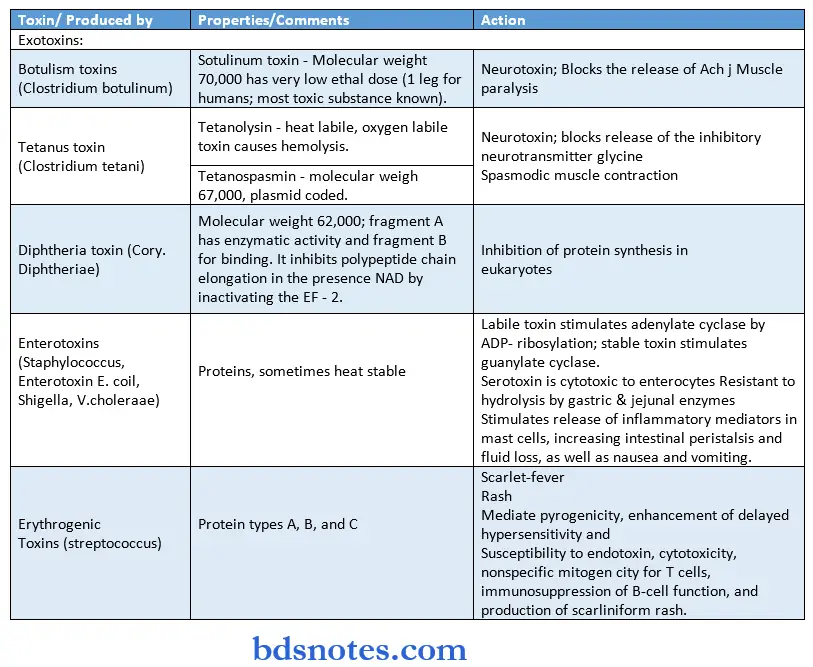
Properties of selected bacterial toxins:
Enzymes secreted by invasive bacteria:
- Coagulase: Staph produces coagulase. It inhibits phagocytosis.
- Fibrinolysins: Promote the spread of infections by breaking down fibrin barriers.
- Hyaluronidase: Splits hyaluronic acid, which acts as a component of an intercellular connective tissue, and facilitates the spread of infection.
- Leucocidins: Damage polymorphonuclear leukocytes.
- Hemolysins: Damage RBCs.
Toxoid:
- Treatment of exotoxins with formaldehyde yields toxoids, which are nontoxic but retain the ability to induce antibodies.
Adhesion:
- Adhesion is a specific reaction between the surface receptor of host cells and adhesion structures on the surface of bacteria.
- These structures are called adhesives, which may occur as “fimbriae” ur “pili”, colonization factors.
Capsule:
- The capsule protects bacteria from deleterious agents and contributes towards virulence by inhibiting phagocytosis.
- It is demonstrated by the serological method.
- When suspension or capsulated bacteria is mixed with specific anti-capsule sera and examined under the microscope, the capsule becomes prominent and appears swollen due to its refractivity.
- This capsular swelling is called (“Quellung’s reaction”).
“Early warning signs of poor performance in microbiology exams: Common questions”
Systemic Bacteriology Staphylococci
Systemic Bacteriology Staphylococci General Characteristics:
- Ubiquitous organisms, medically the most important group and cause major problems in hospitals in compromised patients with debilitating diseases, extensive surgery, immunosuppression, etc.,
- May be part of the normal flora of carriers in the anterior nares, perineum, GIT, skin, etc.
Systemic Bacteriology Staphylococci Physiology and structure:
- Gram-positive cocci arranged in grape-like clusters, non-motile, non-sporing, app Jim diameter.
- Colonies are sharply defined, round, and convex, and grow readily on ordinary media.
- Aerobe and facultative anaerobe
- On mar conkeys agar – very small and pink colonies due to lactose fermentation
- Catalase positive, oxidase negative, ferment glucose and mannitol, producing add but no gas.
- Coagulase (‘clumping factor) positive
- Protein A (useful for identification)
- Capsule
- Species-specific teichoic acid.
Systemic Bacteriology Staphylococci Epidemiology
- Normal flora on human skin and mucosal surfaces.
- Person-to-person spread through direct contact or exposure to contaminated fomites.
- Risk factors include the presence of a foreign body, previous surgical procedures, and the use of antibiotics that suppress the normal microbial flora.
- Patients at risk for specific diseases include menstruating women (TSS), infants (scalded skin syndrome), and children with poor oral hygiene (impetigo) and intravascular catheters (bacteremia).
Systemic Bacteriology Staphylococci Clinical manifestations
- Local or contiguous infections:
- Skin – Folliculitis, boils, carbuncle, impetigo, furuncle
- Eye – styes, conjunctivitis
- Lungs – pneumonia
- Wounds – trauma or surgical sites (sp. Absomen)
Systemic Bacteriology Staphylococci Disseminated infections:
- Through blood stream – osteomyelitis, polyarthritis, Ac. bacterial endocarditis, empyema, pneumonia, catheter-related bacteremia.
- Toxin-associated infections – scalded skin syndrome, food poisoning, Toxic shock syndrome.
- TSS – occurs in females using tampons, characterized by high fever with vomiting and diarrhea, the collapse of peripheral circulation, hypotensive shock, and scarlatiniform rash with desquamation of the skin.
- Food poisoning, enterocolitis, and nosocomial infestations.
Systemic Bacteriology Staphylococci Lab diagnosis:
- Gram-positive, coagulase test & mannitol fermentation confirm the identification of S. aureus,
- Grow rapidly when cultured on nonselective media.
Systemic Bacteriology Staphylococci Treatment, Prevention & Control
- Antibiotics of choice are oxacillin or vancomycin
- The focus of infection must be identified and drained
- Proper cleansing of wounds and use of disinfectant help prevent infections
- Thorough hand washing a covering of exposed skin helps medical personnel prevent infection or spread to others.
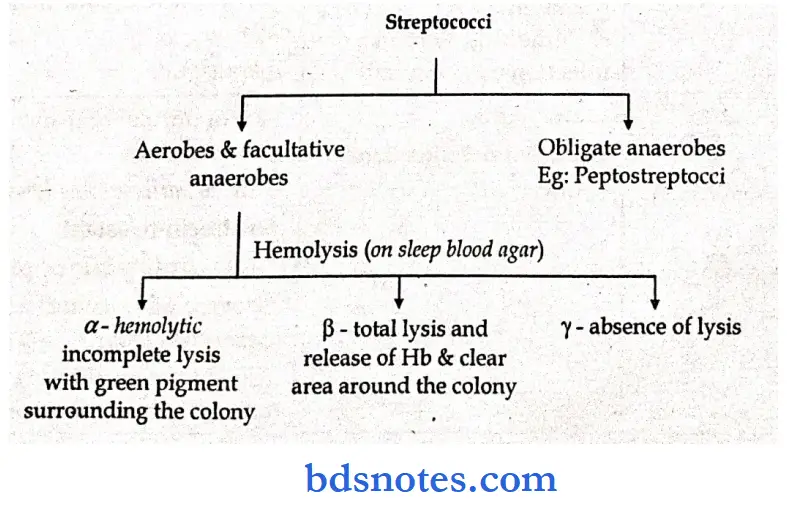
Streptococci General characteristics
- Are a large group of bacteria, heterogenous, facultative anaerobes
- Attach to epithelial surfaces via the lipoteichoic acid portion of fimbriae
- Are classified into groups by serology
“Asymptomatic vs symptomatic effects of outdated study methods: Answered”
Streptococci Morphological features:
- Gram-positive cocci, arranged in long chains, non-motile, non-sporing, app.pm diameter, capsulated
- Colonies are small, motile, semitransparent, grey to greyish white on blood agar
- b-hemolytic, catalase.
- Negative, P& R-positive; bacitracin-susceptible (important identification tests)
- Group specific carbohydrate (A antigen) and type-specific antigen (m. protein) in cell wall
- Produce streptolysin O and DNase B (antibodies against these antigens (ASO, anti-DNase B) are clinically important).
Systemic Bacteriology Staphylococci Epidemiology
- Asymptomatic colonization in URT and transient colonization of skin.
- Person-to-person spread by respiratory droplets or through breaks in the skin after direct contact with an infected person.
- Individuals at higher risk for disease include children 5 to 15 years old (Pharyngitis);
- patients with extensive soft tissue infections and bacteremia (streptococcal toxic shock syndrome); children 2 to 5 years who have poor personal hygiene (Pyoderma); young children and older adults with preesdstmg respiratory tract or skin infections caused by S. pyogenes.
Systemic Bacteriology Staphylococci Diagnosis
- Microscopy is useful in pyogenic infections.
- Direct antigen tests are useful for the diagnosis of streptococcal pharyngitis, but negative results must be confirmed by culture.
- Culture is highly sensitive.
- ASO test is useful for confirming rheumatic fever and acute glomerulonephritis.
- Anti-DNase B test should also be performed if acute glomerulonephritis is suspected.
Systemic Bacteriology Staphylococci Treatment, Control & Prevention
- Penicillin is the drug of choice; erythromycin or oral cephalosporin is used for patients allergic to penicillin.
- Starting antibiotic therapy within 10 days in patients with Pharyngitis prevents rheumatic fever.
- The focus of infection must be identified and drained
- Proper cleaning of wounds and the use of disinfectants help prevent infections.
- For patients with a history of rheumatic fever, antibiotic prophylaxis is required before procedures (e.g., dental) that can induce bacteremias leading to endocarditis.
Systemic Bacteriology Staphylococci General characteristics:
- Is part of the normal flora in 50-70%
- Gram-positive, a-hemolytic, lancet-shaped diplococcus
- Causes more than 80% of all cases of bacterial pneumonia; also meningitis, otitis media, and septicemia.
Systemic Bacteriology Staphylococci Morphological features:
- Capsulated; types are differentiated by swelling of the capsule in the presence of a specific antiserum (quelling reaction)
- Aerobes and facultative anaerobes
- Colonies usually are small, circular, raised, and smooth on blood agar; on prolonged intubation, autolysis occurs, and the center of the colony sinks (draughtsman appearance) due to the presence of an autolytic enzyme (amidase)
- Catalase and oxidase negative
- Large polysaccharide capsule
- Teichoic acid is rich in choline that reacts with a serum protein (referred to as the C-reactive protein) this is a useful diagnostic test for systemic disease.
- Bacteria are inhibited by optochin.
Epidemiology
- Most infections are caused by endogenous spread from the colonized nasopharynx or oropharynx.
- Colonization is highest in young children.
- Person-to-person spread through infectious droplets is rare.
- Individuals with antecedent viral respiratory tract disease or other conditions that interfere with bacterial clearance from, the respiratory tract are at increased risk (or pulmonary disease.
- Children and the elderly are at risk for meningitis.
- People with hematologic disorders are at risk for fulminant sepsis.
“Can advanced tools supplement microbiology note preparation? FAQs provided”
Clinical manifestations
- Pneumonia – Lobar and Bronchopneumonia (one of the most common causes of community-acquired disease)
- Meningitis (The most common cause of bacterial meningitis in most age groups)
- Otitis media and septicemia
Lab diagnosis: Confirmed by biochemical tests performed on a pure culture
- Isolation of Pneumococci
- Fermentation of insulin
- Quellung reaction – Microscopy
- Bile solubility test.
Treatment, Prevention & Control
- Penicillin is the drug of choice for susceptible strains.
- Cephalosporins, erythromycin, chloramphenicol, or vancomycin are used for patients allergic to penicillin or for treatment of penicillin-resistant strains.
- Immunization with 23-valent vaccines can prevent infection.
Neisseria Gonorrhoeae
Neisseria Gonorrhoeae General characteristics
- Is epidemic, with die highest incidence in sexually active age groups (15 – 25)
- Is pyogenic
Neisseria Gonorrhoeae Morphological Features
- Gram-negative cocci (app 2Jim), occur characteristically in pairs (diplococci) with adjacent sides concave (bean shape)
- Usually are intracellular
- Capsulated, non-motile, strict aerobes, piliated
- Colonies are small, round, convex, grey, and translucent on solid media; blood and chocolate agar are commonly used.
- Thayer – Martin and Nezo York City media are selective media
- Catalase and oxidase positive
Neisseria Gonorrhoeae Epidemiology:
- Humans are the only natural hosts
- Asymptomatic carriage is the major reservoir
- Transmission primarily by sexual contact
- The disease is most common in blacks, people aged 15-24 years, (southeastern states), and people who have multiple sexual partners.
- Higher risk of disseminated disease in patients with deficiencies in components of complement.
Neisseria Gonorrhoeae Clinical manifestations
- Urethritis; if complicated epididymitis, prostatitis (in males) and PID (in females) sterility.
- Rectal infections
- Bacteremia, arthritis
- Pharyngitis
- Disseminated infection.
- Infant eye infection (ophthalmia neonatal)
Neisseria Gonorrhoeae Lab diagnosis:
- Gram stain of urethral specimens.
- Culture is sensitive and specific but has been replaced with molecular probe techniques in many laboratories.
- Prevention consists of patient education, the use of condoms or spermicides with nonoxynol (only partially effective), and aggressive follow-up of sexual partners of infected patients.
Neissaeria Meningitis
- Treatment, Prevention & Control
- Ceftriaxone, cefixime, ciprofloxacin, or ofloxacin can be administered in uncomplicated cases.
- For neonates, prophylaxis with 1% silver nitrate; ophthalmia neonatal is treated with ceftriaxone.
- Physiology and structure
- Gram-negative diplococci with fastidious growth requirements.
- Grows best at 35°C to 37°C in a humid atmosphere.
- Oxidase negative and catalase-positive; acids produced from glucose and maltose oxidatively.
- Outer surface antigens include polysaccharide capsules, pili, and lipo oligosaccharides (LOS).
“Differential applications of traditional vs digital note resources: Q&A”
Neissaeria Meningitis Virulence
- Specific receptors for meningococcal pili allow colonization of the nasopharynx.
- Endotoxin mediates most clinical manifestations.
- Causes a highly fulminant disease prevalent at age is 6 months to 24 years
Neissaeria Meningitis Virulence Factors
- Capsular polysaccharide – inhibits phagocytosis
- IPS- cause extensive tissue necrosis, hemorrhage, circulatory collapse, intravascular coagulation, and shock
- IgA ase – degrades IgA.
Neissaeria Meningitis Epidemiology
- Humans are the only natural hosts.
- Person-to-person spread occurs via aerosolization of respiratory tract secretions.
- The highest incidence of the disease is in children younger than 5 years, institutionalized people, and patients with late complement deficiencies.
- Meningitis and meningococcemia are most commonly caused by serogroups B and C; pneumonia is most commonly caused by serogroups Y and W135; serogroup A associated with disease in underdeveloped countries.
- The disease occurs worldwide, most commonly in the dry, cold months of the year.
Neissaeria Meningitis Clinical manifestations: Meningitis
- Begins as mild pharyngitis
- In the susceptible age group, disseminate to most tissues, resulting in fulminant meningococcemia with meningitis features.
- Petechial eruptions with vasculitic purpura are the hall.
- Water house – fridrichsen syndrome is a fulminating disease with hemorrhage, circulatory failure, and adrenal insufficiency.
- Meningoencephalitis
- Bacteremia, pneumonia, arthritis, urethritis.
Neissaeria Meningitis Lab diagnosis
- Gram-negative diplococcus, identify by Gram stain of CSF and skin lesions.
- Culture – Inoculate in nutrient broth or Thayer – martin chocolate agar & incubate in a candle jar
Neissaeria Meningitis Treatment, Prevention & Control
- Breast-feeding infants have passive immunity (first 6 months).
- Treatment is with penicillin (drug of choice), chloramphenicol, ceftriaxone, and cefotaxime.
- Chemoprophylaxis for contacts is with rifampin or sulfadiazine (if the isolated organism is susceptible).
- For immunoprophylaxis, vaccination is an adjunct to chemoprophylaxis; it is used only for serogroups A.
- C, Y, and W135; no effective vaccine is available for serogroup B.
Corynebacterium
Corynebacterium General Features
- Causes disease primarily by elaboration of potent exotoxins.
- The organism does not need to enter the bloodstream to produce systemic signs of disease.
- Is a classic example of lysogenic conversion.
- The tox gene that codes for die exotoxin is introduced into strains of C.
- diphtheria by a lysogenic bacteriophage (fi-phage).
- Is a component of the DTP vaccine.
- Causes disease primarily in infants.
Corynebacterium Cellular morphology
- Slender gram-positive rods that display pleomorphism
- Some strains have club-shaped ends and some have intracellular polyphosphate granules known as metachromatic granules
- Frequently remains attached after division, which gives them a Chinese letter pattern
- Colonies – on serum broth – turbid and pellicle formation
- Loejfler’s serum slope – very rapid growth; small, circular, white or creamy, and glistening
- Tellurite blood agar – gray or black colonies
- Facultative anaerobe.
Corynebacterium Toxin:
- Complications and mortality rates are due to the systemic effects of exotoxin.
- This 53,000 – Da protein is an example of the classic A-B exotoxin.
- Production of exotoxin is the result of the tox + gene carried by a bacteriophage (/page)
- Is a protein consisting of Fr – A – inhibits protein synthesis by binding to and inactivating elongation factors two Fr – B – responsible for toxin attachment to tissues and for transport of Fr – A into the cell.
Corynebacterium Primary effects of the toxin
- Inhibits protein synthesis in the cardiac muscle causing structural and functional damage
- Demyelination – can affect both peripheral and cranial nerves
- Toxin synthesis is regulated by a chromosomally encoded element, diphtheria toxin repressor (DTxR)
Corynebacterium Clinical manifestations
1. Pharyngeal diphtheria:
- Acquired via the respiratory route; pharyngitis and tonsillitis are common pseudomembrane forms as the infection progresses composed of lymphocytes, plasma cells, cellular debris, fibrin, and bacteria greyish white and firmly adherent.
- Cervical lymphadenitis – bull neck appearance
- Complications associated with tissue damage principally at
- Heart cardiac dysfunction, myocarditis, and circulatory collapse
- Nervous system – motor defects result from demyelination; paralysis of throat muscles and polyneuritis
“Steps to incorporate AI into analyzing microbiology notes: Questions and answers”
2. Cutaneous diphtheria
- May present as a simple pustule or chronic non-healing necrotic ulcer.
Corynebacterium Lab diagnosis
- Gram-positive rods; cultured primarily on Loeffler’s medium – cells exhibit a Chinese letter pattern and Babes – Ernst bodies; on Tellurite medium – black or gray colonies.
Corynebacterium Toxin production
- In vitro Elek test involves an antitoxin on filter strips that precipitates with a toxin elaborated from growing organisms.
- In vivo animals are injected with a toxin-containing culture citrate, then an antitoxin to demonstrate protection.
- Demonstration of exotoxin is performed by molecular or immunologic methods.
Corynebacterium Treatment
- Antitoxin is administered immediately (i.m) to neutralize exotoxin.
Corynebacterium Microbiology
- Antimicrobial therapy (Erythromycin) may help reduce the number of Cdiphtheriae.
- Prevention – treatment of D. toxin with formalin produces a non-toxic, immunogenic substance (toxoid – generates antibodies, that neutralize the toxin) that is usually administered throughout early childhood, as part of the diphtheria, tetanus, and pertussis vaccine (DTP).
- Booster immunizations at 10-year intervals maintain immunity.
The Schick test determines immune status Inject the toxin and heated toxin dermally at different sites:
- At the toxin site, if maximum erythema occurs after 5 days, the patient is non-immune; if no erythema occurs after 5 days, the patient is immune
- At the heated toxin site, if some erythema occurs after 1 to 2 days and then disappears, the patient is hypersensitive to the toxin, if no erythema occurs after 1 to 2 days, the patient is not hypersensitive.
- Gram- Negative Bacilli
Characteristics Of Major Groups Of Gram-negative Rods:
- General characteristics
- Composed of hundreds of closely related species inhabiting the large bowel of humans and animals.
- Causes two major disease syndromes: nosocomial infections and GIT disturbances.
- Morphology
- Gram-negative bacilli, non-spore-forming, encapsulated, facultative anaerobes that ferment glucose.
- Colonies – typical colonies are circular, convex, and glistening of mucoid.
- The loss of capsules produces rough colonies that are flat, irregular, and granular.
- Surface components & antigens of Enterobacteriaceae
Flagella
- Composed of contractile fibrous proteins (flagellins)
- Constitute tire H angitens (H = Hauch) (German) = Breath)
- Preserved by formalin, destroyed by heat
- Maximal in young cultures
Fimbriae (pili):
- Hair-like projections of protein on cell surface, promote adhesion
- Develop in old (24 – 48 hr) broth cultures
- Destroyed by heat, preserved by formalin
- Six types are described, according to their ability to agglutinate red cells.
- May interfere with H agglutination
Capsule:
- A thin layer of surface polysaccharide constitutes the K antigen (K = Kapseal (German) – capsule)
- The formation is enhanced by sugar-containing media
- Very prominent in klebsiella, in which as a loosely adherent slime layer, it creates mucoid colonies
- May interfere with agglutination
- Inhibits phagocytosis
- May cross-react with capsular antigens of other bacteria Cell wall consists of two layers:
1. Outer layer: a complex of Lipopolysaccharide (LPS), protein, and lipids, which render Gram-negative cells less permeable to solutes.
- The side chains of repeating sugar units project from the outer LPS layer constituting the O antigen (O = Ohne (German) = without).
- Associated with smooth colonies, resistance to killing by complement.
- The absence of side chains is associated with rough colonies, auto-agglutination, nonvirulence, and killing by complement.
- Core glycolipids form the basal layer to which side chains are attached (the enterobacterial common antigen)
- Lipid A forms a layer between the lipopolysaccharide and a Phospholipid membrane.
- Is the toxic moiety of ‘endotoxin”
- Phospholipid membrane is similar in structure to the tire cell membrane (and therefore termed the ‘outer membrane’)
- Proteins (outer membrane proteins, OMPs) are present in tire phospholipid membrane.
- They include those responsible for solute transport (porins) and c-structural lipoproteins.
- The inner layer of the cell wall consists of peptidoglycan maintaining cell rigidity.
Exotoxins:
- Enterotoxins: Produced by some strains of Esch. Colt & probably other Enterobacteriaceae.
- Cytotoxins: Sh. dysenteriae and some strains of Esch. Coli.
“Role of digital tools in improving precision with microbiology note-taking: FAQs explained”
E.Coli
- Physiology and structure
- Gram -negative bacilli
- facultative anaerobe
- Fermenter
- oxidase negative.
- Oxidase negative.
- The outer membrane makes tiny organisms susceptible to drying.
- Lipo polysaccharide consists of outer somatic polysaccharide, core polysaccharide (common antigen), and lipid A (endotoxin).
- Virulence factors
- Capsule – suppresses phagocytosis
- Endotoxin (LPS) – heat stable, composed of three components – Lipid A, the core polysaccharide, and the somatic O antigen, Lipid A moiety is responsible for most of the symptomatology.
- Endotoxic shock – is initiated by endotoxin and consists of fever, leucopenia, hypoglycemia, hypotension and shock, DIC, and death from massive organ dysfunction.
- Exotoxins – Heat – stable STa & STb, Hemolysin, Heat labile toxin LJ-1 & LJ-1
- Adhesion colonization factors – involved in surface interactions of bacteria and conjugation
- Antimicrobial resistance – is fed on transferable plasmids.
- Invasive capacity,
Exotoxins Epidemiology
- Most common aerobic, Gram-negative bacilli in the gastrointestinal tract.
- Most infections are endogenous (patient’s normal microbial flora).
- Strains causing gastroenteritis are generally acquired exogenously.
Exotoxins Diseases
- Bacteremia (most commonly isolated gram-negative bacillus)
- Urinary tract infection (the most common cause of bacterial UTl’s); is limited to bladder (cystitis) or can spread to the kidneys (pyelonephritis) or prostate (prostatitis).
- Neonatal meningitis (usually with strains carrying the K1 capsular antigen).
- Intra-abdominal infections (associated with intestinal perforation).
- E. coli, a prominent member of the indigenous flora of the human intestinal tract, also is a major etiologic agent in urinary tract infection and gastroenteritis.
- Ascending urinary tract infection: is caused most commonly by E, coli, and the disease may progress from simple urethritis to serious pyelonephritis.
- It is characterized by dysuria, frequency of urination, pyuria, and occasionally hematuria.
Gastroenteritis
- caused by E. coli ranges from simple diarrhea to a more severe form with a debilitating loss of fluids and electrolytes.
- Gastroenteritis is most serious and sometimes fatal in nutritionally deprived infants and elderly debilitated adults.
- Enterotoxigenic E. coli produces one or both of two enterotoxins that are coded for by genes residing on a transmissible plasmid.
- One toxin is heat labile and the other is heat stable.
- The heat-labile toxin causes diarrhea by the same mode of action as cholera enterotoxin.
- The toxin binds to ganglioside receptors of the intestinal mucosa and other cells, and it activates membrane-bound adenyl cyclase.
- Increased intracellular concentrations of cyclic adenosine 3′, 5′-
- monophosphate (cAMP) causes the active excretion of electrolytes, which carry large amounts of water with them.
- Heating at 65° C for 30 minutes can destroy the heat-labile toxin.
- The heat-stable toxin: causes diarrhea by stimulating guanyl cyclase in intestinal mucosal cells only.
- The receptor for this toxin is unknown, but it is obviously unique to susceptible cells.
- The heat-stable toxin is a small, heterologous polypeptide molecule; it is not destroyed by heating at 100°C for 30min.
- Enteroinvasive E.coli causes diarrhea by invading the intestinal epithelial cells and eliciting an inflammatory response.
- The exact cause of the diarrhea is known, but it may be due to the cytotoxic effects of lipopolysaccharide.
Gastroenteritis Diagnosis
- Organisms grow rapidly in most culture media.
- Treatment, Prevention, and Control
- Infections are controlled by the use of appropriate infection-control practices to reduce the risk of nosocomial infections.
- Maintenance of high hygienic standards to reduce the risk of exposure to gastroenteritis strains.
- Proper cooking of beef products to reduce the risk of EHEC infections.
- Gastroenteritis is caused by different strains of Esch. Coli
- septicemia and pyogenic -may cause wound infection, peritonitis, biliary tract infections, and neonatal meningitis
“How do advancements in technology enhance microbiology note preparation? Q&A guide”
Salmonella General characteristics
- Most human disease results from salmonella typhi, salmonella enteritidis, salmonella typhimurium, salmonella paratyphi A, salmonella schottmiilleri, or salmonella choleraesuis.
- Do not ferment lactose, but many species are Identified by the production of add, gas, and hydrogen sulfide from glucose
Salmonella Physiology and Structure:
- Gram-negative bacilli,
- Facultative anaerobe,
- Oxidase-negative.
- Lipo-polysaccharide consists of outer somatic polysaccharide, core polysaccharide (common antigen), and lipid A (endotoxin).
Salmonella Attributes of pathogenicity (virulence factors)
- Possess an endotoxin causing diverse toxic manifestations, including fever, leukopenia, hemorrhage, hypotension, shock, and DIC.
- May possess an exotoxin (enterotoxin)
- Are aided by the anti-phagocytic activity of the capsule.
- Can survive within macrophages by unknown means.
Salmonella Epidemiology
- Most infections are acquired by eating contaminated food products (poultry, eggs, and dairy products are the most common sources of infection).
- Direct fecal-oral spread in children.
- S, typhi, and S. paratyphi are strictly human pathogens (no alternative reservoir); these infections are passed from person to person; asymptomatic long-term colonization occurs commonly.
- Individuals at risk for infection include those who eat improperly cooked poultry or eggs, patients with reduced gastric add levels, and immuno-compromised patients.
- Infections occur worldwide, particularly in the warm months of the year.
Salmonella Clinical Diseases:
- Enterocolitis: (Gastroenteritis or food poisoning)
- Is currently the most common form of salmonella infection in the united states (approximately two million cases per year).
- Occurs in multiple sources of contamination, including food, most commonly poultry and poultry products, human carries (particularly food handlers), exotic pets (turtles and snakes).
- Is commonly caused by S.typhimurium and S.enteritidis, which usually require a high infecting dose with an 8- 48 hours incubation period.
- Is a self-limiting illness manifested by fever, nausea, vomiting and diarrhea.
- May have an increased carrier rate with antibiotic therapy.
- Is usually characterised by the following pattern.
- Ingestion of organisms in contaminated food.
- Colonization of the ileum and cecum.
- Penetration of epithelial cells in the mucosa and invasion, resulting in acute inflammation and ulceration.
- Release of prostaglandin by enterotoxins, resulting in activation of adenyl cyclase and increased cyclic AMP.
- Increased fluid secretion in the intestines.
Septicemic (Extraintestinal) Disease:
- Is an acute illness most often of nosocomial origin, with abrupt onset and early invasion of the bloodstream.
- Is characterized by a precipitating incident that introduces bacteria (e.g., catheterization, contaminated IV fluids, abdominal or pelvic surgery), followed by a triad of chills, fever, and hypotension.
- May cause local abscess, osteomyelitis, and endocarditis if the organisms are disseminated widely.
- May be caused by many Salmonella species as well as other Enterobacteriaceae organisms.
- Has a high mortality rate (30-50%), depending on the degree of preexisting debilitation.
Septicemic Enteric fevers:
- Are produced mainly by S. typhi (typhoid fever) and a lesser degree by S. paratyphi and S.schottmulleri, all of which are strictly human pathogens.
- Occur through ingestion of food or water, usually contaminated by an unknowing carrier,
- Are highly infective even with small numbers of bacteria (e.g, 200)
Septicemic Progress as follows:
- During an incubation period of 7 – 14 days, the organisms multiply in the small intestine, enter the intestinal lymphatics & are disseminated via the bloodstream to multiple organs.
- Blood cultures then become positive & the patient experience malaise, headache & gradual onset of a fever that increases during the day, reaching a plateau of 102° -105°F each day,
- Multiplication takes place in the reticuloendothelial system and lymphoid tissue of the bowel, producing hyperplasia and necrosis of the lymphoid Peyer’s patches.
- A characteristic rash (“rose spots”) appears in the 2nd to 3rd week in about 90% of patients.
- Typically the disease lasts 3-5 weeks, the major complications are gastrointestinal hemorrhage and bowel perforation with peritonitis.
- Following recovery, 3% of patients become carriers; the organism is retained in the gallbladder and biliary passages, and cholecystectomy may be necessary.
“Early warning signs of outdated methods in microbiology note studies: Common questions”
Septicemic Laboratory diagnosis:
- Enterocolitis: blood cultures are usually negative, and agglutination reactions are not helpful.
- Septicemic disease: diagnosis is usually by blood culture because the organisms do not localize in the bowel and stool cultures are often negative.
- Enteric fevers: diagnosis is by isolation of the organism from the blood or stool after 1-2 weeks by plating onto differential media, selective media, or both.
- Diagnosis by serology, showing rising titers of O antibody, is of lesser significance.
- Treatment, Prevention, and Control
- Infections with S. typhi and S.
- paratyphoid or disseminated infections with other organisms should be treated with an effective antibiotic.
- Fluoroquinolones (e.g., ciprofloxacin), chloramphenicol, trimethoprim; sulfamethoxazole, or a broad-spectrum cephalosporin can be used.
- Most infections can be controlled by proper preparation of poultry and eggs (completely cooked) and avoidance of contamination of other foods with uncooked poultry products.
- Carriers of S. typhi and S. paratyphi should be identified and treated.
- Vaccination against S. typhi can reduce the risk of disease for travelers into endemic areas.
Septicemic General characteristics:
- Is a gram-negative, facultatively anaerobic, non-motile rod.
- All Shigella species are pathogenic in small numbers for humans.
- Have no known animal reservoir and are not found in soil or water unless contaminated with human fecal material.
- Perpetuation of Shigella-induced disease is due largely to unrecognized clinical cases and convalescent and healthy carriers, less than 1% of whom are under the care of a physician.
- The disease spreads through poor sanitation and is readily transmitted from person to person via food, fingers, feces, and flies.
- All Shigella species ferment glucose with acid, but rarely with gas; only Shigella sonnei ferments lactose.
Septicemic Classification:
- Is classified into four groups based on differences in somatic (O) antigens:
- Group A: Shigella dysenteriae (rarely found in the united states, unless imported).
- Group B: Shigella flexneri (common in the united states)
- Group C: Shigella boydii (rarely found in the united states)
- Group D: Shigella sonnei (the most common cause of shigellosis in the united states)
Septicemic Virulence attributes:
- All Shigellae contain an endotoxic LPS.
- destruction and ulceration.
- Endotoxin and genes for adherence, invasion, and intracellular replication.
- Permeability barrier of the outer membrane.
- Organisms possess the capacity to multiply intracellularly, resulting in focal.
- Exotoxin (Shiga toxin) is produced by S. dysenteriae; disrupts protein synthesis and produces endothelial damage.
- Hemolytic colitis (HC) and hemolytic uremic syndrome (HUS) associated with Shigella,
Septicemic Epidemiology:
- Humans are the only reservoir for these bacteria.
- Disease spread person-to-person by fecal-oral route.
- Patients at the highest risk for the disease are young children in daycare centers, nurseries, and custodial institutions; siblings and parents of these children; male homosexuals.
- Relatively few organisms can produce disease (highly infectious).
- Disease is worldwide with no seasonal incidence.
Septicemic Clinical disease:
- Shigellosis (bacillary dysentery) is characterized by acute inflammation of the wall of the large intestine and terminal ilium; bloodstream invasion is rare.
- Complications include necrosis of the mucous membrane, ulceration, and bleeding.
- The disease is characterized by a sudden onset after a short incubation period (1-4 days), with abdominal pain, cramps, diarrhea, and fever.
- Stools are liquid and scanty; after the first few bowel movements, they contain mucus, pus, and occasionally blood.
“Asymptomatic vs symptomatic effects of ignoring new trends in microbiology notes: Answered”
Septicemic Laboratory diagnosis:
- Is made from stool culture of the organism into differential and selective media.
- Cannot be made by using serology and blood culture.
- Treatment, Prevention and Control.
- Antibiotic therapy shortens the course of symptomatic disease and fecal shedding.
- Empiric therapy can be initiated with fluoroquinolone or trimethoprim; or sulfamethoxazole.
- Appropriate infection control measures should be instituted to prevent the spread of the organism, including hand washing and proper disposal of soiled linens.
- Only Sdycnteriae infections require antibiotic therapy; however resistance to antibiotics has been developing,
- Fluid replacement is the most important therapy.
- Vaccines are under development,
- Epidemiologic control by isolation of carriers, disinfection of excreta, and proper sewage disposal can be effective.
Septicemic General characteristics
- Cholera is one of the most devastating diseases; the pandemic last for years; Prototype of enterotoxin-induced diarrhea.
- A large and rather poorly characterized group of Gram-negative rods, mainly environmental, especially in marine and brackish waters.
- Tolerate high salt concentrations (i.e. halophilic).
- Curved rods, single polar flagellum. Oxidase positive, catalase positive.
Fermentative
- Species of medical interest
- Vibrio cholera: Includes 72 serotypes, one of which (01) causes epidemic cholera
- Vibrio parahaemolyticus: Causes gastroenteritis (from seafood)
- Vibrio alginolyticus: Occasionally causes wound infection following wounds sustained in seawater
- Vibrio: Occasionally causes septicemia after eating raw oysters
- Vibrio group F (EF-6): Has been recently described as a cause of gastroenteritis.
- Virulence factors of Vibrio cholerae 01 and 0139
- Vibrio species: are small, curved, gram-negative rods that are motile by means of a single polar flagellum.
- The genus includes two important human pathogens.
Fermentative Physiology and Structure
- Curved Gram-negative bacilli.
- Facultative anaerobe.
- Fermenter.
- Simple nutritional requirements do not require salt for growth but can tolerate it.
- Strains are subdivided by their O cell wall antigens.
- Two biotypes of V. cholerae Ol strains – El tor and classical (this is important for epidemiologic classification of isolates).
- Vibrio cholera: is the etiologic agent of human cholera, a diarrhea syndrome that can be fatal owing to a severe loss of water and electrolytes.
- Antigenic composition and Biochemistry
- The bacterium is similar bio-chemically to the Enterobacteriaceae, except that it is oxidase-positive & grows most efficiently at a pH level of 9.0 – 9.5.
- Serotyping is based on the antigens; three major serotypes – the Ogawa, Inaba, and El for strains – have been placed in serogroup O type (i.e. 0:1).
- These three strains are capable of producing severe diarrhea.
Fermentative Epidemiology:
- Cholera is spread by the ingestion of fecally contaminated food & water.
- Direct person-to-person spread is rare because the infectious dose is high because stomach acids kill most organisms.
- The nutritional status of infected people may play an important role in the disease.
- Those with an alkaline pH in the stomach and intestines appear to be more easily infected.
- The disease is prevalent in far India, the Middle East, and Africa.
- A few cases occur annually in the United States.
- Organisms responsible for major pandemics (worldwide epidemics), with significant mortality in underdeveloped countries.
- All pandemics of cholera are caused by serotype 01, although 0139 can cause a similar disease and may cause a pandemic.
- Bacterial levels increase in contaminated water during the warm months.
“Differential applications of traditional vs cutting-edge microbiology note techniques: Questions answered”
Fermentative Pathogenicity:
- V.cholerare colonizes the intestinal tract in very high numbers.
- The cells attach to but do not invade intestinal mucosa.
- A potent enterotoxin is released and binds to ganglioside receptors on the mucosal cells.
- After a lag period of 15-45 minutes, adenyl cyclase is activated and the camp concentration inside the intestinal cells increases.
- Increased intracellular cAMP results in the excretion of electrolytes such as chloride and bicarbonate ions along with massive quantities of water.
Fermentative Symptomatology:
- The major symptom of cholera is diarrhea.
- The feces contain epithelial cells, mucus, and large numbers of V.cholerae.
- The presentation can range from mild disease to severe life-threatening disease.
- The disease is characterized by profuse watery diarrhea (rice water stools).
- In severe cases, as much as one liter of fluid may be lost each hour.
- The patient usually feels bloated and may have abdominal pain before the onset of diarrhea.
- Death is caused by electrolyte abnormalities and massive fluid loss.
Fermentative Laboratory diagnosis:
- V.Cholerae may be viewed directly in stool samples, particularly in dark-field microscopy.
- Fluorescently labeled antibodies can be used in identifying the observed cells as V.cholerae.
- Selective media for culture are based on the ability of vibrios to grow at an alkaline pH, and identification can be made by biochemical tests.
- Treatment, Prevention, and Control
- Intravenous administration of fluids and electrolytes is critical for recovery.
- Oral administration of a solution containing glucose and electrolytes has been successful, but the patient must be capable of consuming the liquid by mouth.
- Severely ill patients generally are too weak to ingest fluids.
- Antibiotic therapy does not affect the disease once, the enterotoxin attaches to the intestinal cells, but can prevent later attacks by reducing the number of toxin-producing V.cholerae in the intestines,
- Doxycycline (adults), trimethoprim-sulfamethoxazole (children), or furazolidone (pregnant women) is administered.
- Improved hygiene is critical for control.
- Immunization: with toxoids, live cells or attenuated cells provide only limited protection for approximately six months.
- Vibrio parahaemolyticus is a marine vibrio that requires a relatively high salt concentration for growth.
Fermentative Epidemiology:
- V.parahaemolyticus is distributed worldwide in marine environments and now is recognized as a common etiologic agent of acute enteritis associated with the consumption of improperly cooked seafood.
- The bacterium accounts for about half of all of the above cases of food poisoning in Japan.
- The best control measure is the consumption of only cooked seafood.
Fermentative Pathogenicity:
- The enterotoxin of V. V.parahaemolyticus has not been characterized completely.
- All strains, isolated from cases of gastroenteritis are capable of producing a heat-stable hemolysin that lyses human and rabbit erythrocytes.
- The hemolysis has been designated kanawaga hemolysis, the enterotoxigenic strains are referred to as Kanawaga-positive V.parahaemolyticus.
Fermentative General characteristics
- Pseudomonas Aeruginosa
- Is a small, polarly flagellated, gram-negative rod with pilL
- Is an aerobe and, unlike enterobacteria, is oxidase positive.
- Nonfermenter.
- Simple nutritional requirements.
- Mucoid exopolysaccharide capsule
- Is a small, polarly flagellated, gram-negative rod with pilL
- Is an aerobe and, unlike enterobacteria, is oxidase positive.
- Nonfermenter.
- Simple nutritional requirements.
- Mucoid exopolysaccharide capsule
Morphology
- Slender, gram-negative bacillus, non-capsulated, non-sporing.
- Colonies are smooth, large, translucent, and convex with a sweetish aromatic odor and a blue-green-pigmented surrounding colony.
- Cytotoxin (leukocidin) – cytotoxic for eukaryotic membranes, (disrupts leukocyte function).
Morphology Invasive factors include:
- Pili, which attach to the damaged basement membrane of cells.
- Phospholipase – Heat-labile hemolysin; mediates tissue damage
- Collagenase and elastase – the destruction of elastin-containing tissues (blood vessels, lung tissue, skin) – collagen and complement factors.
- Flagella, to promote motility.
Morphology Virulence factors include:
- Lipopolysaccharide – Endotoxin activity
- Exotoxin A, an adenosine diphosphate (ADP) ribose transferase similar to diphtheria toxin, inactivates the tRNA elongation factor (EF-2), halts protein synthesis and causes liver necrosis.
- Exotoxin S is an ADP – ribose transferase capable of inhibiting eukaryotic protein synthesis.
- Clinical manifestations:
- Is most common in the presence of neutropenia, prolonged antibiotic use, severe burns, cystic fibrosis, trauma/ metabolic disease, or inhalation of large numbers of organisms (such as from contaminated respiratory therapy fluids).
- Is generally accompanied by symptoms of endotoxic shock, DIC and respiratory distress syndrome.
- Frequently begins with overgrowth of Pseudomonas organisms in the intestine of hospitalized patients receiving antibiotics.
- May occur in any site of the body.
Cellulitis
- Occurs in patients with bums, wounds, or neutropenia.
- Is indicated by blue-green pus and a grape-like, sweet odor.
- May be highly necrotic.
Pneumonia
- Mucoid strains may colonize in the lungs in patients with cystic fibrosis.
- May occur in patients exposed to high levels of Pseudomonas organisms in contaminated inhalation therapy equipment.
- Often results in mental confusion, gram-negative septic shock, and cyanosis of increasing severity.
Sephcemiai
- Results from hematogenous spread of the infection from local lesions,
- Results in ecthyma gangrenosum, where dermal veins and tissues are invaded.
- Other opportunistic Pseudomonas infections:
- Urinary tract infections: these are generally chronic and occur in the elderly.
- Endocarditis: in drug addicts.
Sephcemiai Melioidosis:
- May initially go undiagnosed and be followed years later by fulminant septicemia.
- Is caused by P. pseudomallei. UTI, external otitis, (vary from mild ‘swimmers car ‘ to malignant otitis externa), eye infection.
Sephcemiai Laboratory diagnosis
- Is most commonly made by clinical suspicion [grape-like odor, blue-green pus, or ecthyma gangrenosum of gram-negative septicemia) and confirmed by culture.
- Shows p-hemolysis on blood agar with pigment production for most strains.
- Treatment, Prevention, and Control
- Is difficult because of frequent resistance to antibiotics.
- Requires combination therapy (amino glycoside) & an anti-pseudominal p-lactam agent until drug susceptibilities are determined.
- Hyperimmune globulin and granulocyte transfusions may be beneficial in selected infections in immunocompromised patients.
- Hospital infection control efforts should concentrate on preventing contamination of sterile medical equipment and nosocomial infections.
Chlamydia General characteristics
- Are obligate intracellular parasites (cannot synthesize ATP)
- Have a rigid cell wall, which lacks N-acolyte mu ramie add
- Resemble gram-negative bacteria.
Exist in two forms:
- An elementary body, which is infectious A reticular body, which is the intracellular reproductive form
Chlamydia Classification:
- Chlamydia psittaci causes disease in birds {ornithosis), particularly psittacine birds {such as parrots), which causes human respiratory tract infections.
- Chlamydia trachomatis is differentiated into 15 serotypes.
- Chlamydia pneumonia.
- Developmental cycle
- Elementary body – is the extracellular infectious particle,
- Initial body – metabolically active, undergoes binary fission and later forms elementary bodies.
Chlamydia Clinical manifestations:
- Causes a wide spectrum of human respiratory diseases, ranging from sub-clinical infections to fatal pneumonia.
- Causes infection with a sudden onset that initially resembles influenza.
Chlamydia Trachomatis Subtypes A, B, and C:
- Cause chronic keratoconjunctivitis (trachoma) that can progress to conjunctival and corneal scarring and blindness
- Are frequently accompanied by a concomitant secondary bacterial infection.
- Cause neonatal pneumonia
- Subtypes D-K
- Cause a sexually transmitted disease, that may involve an associated inclusion conjunctivitis
- Are a prominent cause of non-gonococcal urethritis in males and urethritis, cervicitis, salpingitis, and pelvic inflammatory disease in females.
- Produce a relatively high incidence of asymptomatic or relatively inapparent infections
- Usually can produce self-limiting inclusion conjunctivitis in infants delivered through an infected birth canal
- May cause neonatal pneumonia.
Chlamydia Subtype:
- Causes a sexually transmitted disease called lymphogranuloma venereum, which is characterized by suppurative inguinal adenitis.
- Lymphadenitis may progress to lymphatic obstruction and rectal strictures if the disease is untreated.
“Can bioinformatics revolutionize microbiology note classification? FAQs provided”
Pneumonia
- Causes various lower respiratory tract infections, including bronchitis and pneumonia.
- Laboratory diagnosis Identification
- Most diseases are diagnosed clinically (typically on the basis of eye damage and urogenital vesicles)
- Fluorescent monoclonal antibodies may be used to stain elementary bodies in exudates:
- Pneumonitis requires organism isolation accompanied by fluorescent antibody stain or complement fixation testing for antibodies.
Pneumonia Clinical specimens:
- Obtain appropriate scrapings or exudates from the eye or urogenital tract
- Obtain sera or tears for serologic testing.
Microbiology Treatment
- Forms spores but they are rarely seen in clinical specimens or culture.
- Replicates rapidly, so large spreading colonies are seen within the first day of culture; “double zone” of hemolysis on blood agar (due to a and S toxins).
- Produces many toxins and hemolytic enzymes, so white blood cells are not seen in gram-stained clinical specimens.
- Produces lecithinase (phospholipase C).
- Subdivided into 5 types (A-E) on the basis of toxin production.
Virulence:
- Spore formation,
- Botulinum toxin (prevents the release of neurotransmitter acetylcholine)
- Binary toxin.
- Epidemiology
- Ubiquitous; present in soil, water, and intestinal tract animals.
- Type A is responsible for most human infections (also the only type capable of surviving in soil).
- The disease follows exogenous or endogenous exposure.
Diseases:
- Soft tissue infections (cellulitis, suppurative myositis, myonecrosis).
- Food poisoning.
- Septicemia.
Diagnosis:
- Characteristic forms are seen on gram stain.
- Grows rapidly in culture,
- Treatment, Prevention, and Control
- Rapid treatment is essential for serious infections.
- Systemic infections require surgical debridement and high-dose penicillin therapy.
- Treat with debridement of arid penicillin for localized infections.
- Antiserum against a toxin not used now, and the value of hyperbaric oxygen treatment is unproven.
- Symptomatic treatment for food poisoning.
- Proper wound care and judicious use of prophylactic antibiotics will prevent most infections
Physiology and Structure:
- Strict anaerobe (vegetative cells are extremely oxygen-sensitive)
- Difficult to isolate from clinical specimens.
Virulence
- Spore formation.
- Tetanospasmjn (heat-labile neurotoxin; blocks release of neurotransmitters [i.e„ gamma-aminobutyric acid, glycine] for inhibitory synapses)
- Tetanolysin (heat-stable hemolysin of unknown significance)
Virulence Epidemiology:
- Ubiquitous; spores are found in moist soils and can colonize the gastrointestinal tract of humans and animals.
- Exposure to spores is common, but the disease is uncommon except in underdeveloped countries, where there is poor vaccination compliance and medical care is inadequate.
- Risk is greatest for people with inadequate vaccine-induced immunity; disease does not induce immunity.
Virulence Microbiology:
- Generalized tetanus (most common form),
- Cephalic tetanus (high mortality),
- Localized or wound tetanus (good prognosis),
- Neonatal tetanus (high mortality),
- Clinical manifestations of Tetanus
Virulence Diagnosis:
- Diagnosis is based on clinical presentation.
- Microscopy and culture with poor sensitivity.
- Neither tetanus toxin nor antibodies are typically detected.
- Treatment, Prevention, and Control
- Treatment requires debridement, antibiotic therapy (metronidazole), passive immunization with antitoxin globulin, and vaccination with tetanus toxoid.
- Prevention through use of vaccination, consisting of three doses of tetanus toxoid followed by boosters every 10 years.
Virulence Physiology and Structure:
- Gram-positive, spore-forming bacillus.
- Strict anaerobe (vegetative cells extremely oxygen-sensitive),
- Fastidious growth requirements.
- Can produce one of seven distinct botulinum toxins (A-G).
- Strains associated with human disease produce lipase, digest milk proteins, hydrolyze gelatin, and ferment glucose.
Virulence
- Spore formation.
- Botulinum toxin (prevents the release of neurotransmitter acetylcholine).
- Binary toxin.
Virulence Epidemiology:
- Ubiquitous; C. botulinum spores are found in soil worldwide.
- Human diseases associated with toxins A, B, E, and F. Relatively few cases of botulism in the United States.
- Infant botulism is more common than other forms.
Virulence Diseases:
- Food borne botulism.
- Infant botulism.
- Wound botulism.
Virulence Diagnosis:
- Botulism is confirmed by isolating the organism or detecting the toxin in food products or the patient’s feces or serum.
- Treatment, Prevention, and Control
- Treatment involves administration of metronidazole or penicillin, trivalent botulinum antitoxin, and ventilatory support.
- Spore germination in foods is prevented by maintaining food at an acid pH, by high sugar content (e.g., fruit preserves), or by storing the foods at 4° C or colder.
- The toxin is heat-labile so can be destroyed by heating food for 20 minutes at 80° C.
- Infant botulism is associated with the consumption of contaminated foods (particularly honey).
- Infants younger than 1 year should not be given honey or foods containing it.
Virulence Physiology and Structure:
- Weakly gram-positive, strongly add-fast, aerobic bacilli. Lipid-rich cell wall, making the organism resistant to disinfectants, detergents, common antibacterial antibiotics, and traditional stains.
Virulence
- Capable of intracellular growth on inactivated alveolar macrophages.
Virulence Epidemiology:
- Worldwide; one-third of the world population is infected with this organism.
- Sixteen million existing cases of disease and 8 million new cases each year.
- The disease is most common in southeast Asia, sub-Saharan Africa, and Eastern Europe.
- Approximately 20,000 new cases in the United States annually.
- Populations at greatest risk for the disease are immuno-compromised patients (particularly those with HIV infection), drug or alcohol abusers, the homeless, and individuals exposed to disposed of patients.
- Humans are the only natural reservoir.
- Person-to-person spread by infectious aerosols.
Virulence Diseases:
- The primary infection is pulmonary.
- Dissemination to any body site occurs most commonly in immunocompromised patients and untreated patients.
Virulence Diagnosis:
- Microscopy and culture are sensitive and specific. Direct detection by molecular probes is relative insensitive.
- Multiple-drag regimens and prolonged treatment are required to prevent development of drug-resistant strains.
- Regimens recommended for treatment include isoniazid and rifampiem for 9 months, with pyrarinmnidc and ethambutol or streptomycin added for drag-resistant strains.
- Prophylaxis for exposure to tuberculosis can include isoniazid for 9 months, rifampiem for 4 months, or rifampin and pyiminamide for 2 months.
- Pyrazinarnide and ethambutol or Ievoflcxadn are used for 6 to 12 months following exposure to drug-resistant M. tuberculosis.
- Immunoprophylaxis with BCG in endemic countries.
Virulence Physiology and Structure:
- Weakly gram-positive, strongly add-fast bacilli,
- Lipid-rich cell wall.
- Unable to be cultured on artificial media.
- Diagnosis made with specific skin test (tuberculoid form) or add-fast stain (lepromatous form).
Virulence
- The disease primarily from the host’s response to infection,
Virulence Epidemiology:
- Rare in the United States but common in other countries (eg., Asia, Africa).
- Armadillos are naturally infected and represent an indigenous reservoir.
- The lepromatous form of the disease, but not the tuberculoid form, is highly infectious.
- Person-to-person spread by direct contact or inhalation of infectious aerosols.
- People in close contact with patients who have lepromatous disease are at greatest risk.
Virulence Diseases:
- Tuberculoid form of leprosy,
- Lepromatous form of leprosy.
- An intermediate form of leprosy,
Virulence Diagnosis:
- Microscopy is sensitive for the lepromatous form but not the tuberculoid form,
- Skin testing is required to confirm tuberculoid leprosy. Culture cannot be used.
- Treatment, Prevention, and Control
- Dapsone with or without rifampin is used to treat the tuberculoid form of the disease; clofazimine is added for the treatment of the lepromatous form.
- Therapy is prolonged.
- Dapsone is recommended for long-term prophylaxis in treated patients.
- The disease is controlled through the prompt recognition and treatment of infected people.
Virulence Physiology and Structure:
- Thin, coiled spirochete, 0.1 x 5 to 15 jam.
- Cannot be seen with Gram or Giemsa stains; observed by dark field microscopy.
- Cannot be grown in vitro except in selected cultured cells.
Virulence factors:
- Outer membrane proteins promote adherence to host cells.
- Hyahrrorddase may facilitate perivascular infiltration.
- Coating of fibronectin protects against phagocytosis.
- Tissue destruction primarily results from host’s immune response to infection.
Virulence Epidemiology:
- Humans are the only natural host.
- Venereal syphilis is transmitted by sexual contact or congenitally; patients at risk include sexually active adolescents and adults, and children born of mothers with active disease.
- Other treponema infections are transmitted by contact of mucous membranes with infectious lesions; congenital infections are rare; patients at risk are children or adults in contact with infectious lesions.
- Venereal syphilis occurs worldwide, endemic syphilis (bejel) occurs in desert and temperate regions of north Africa, the middle east, and northern Australia; yaws occurs in tropical or desert regions of Africa, South America, and Indonesia; pinta occurs in tropical areas of Central and South America.
- No seasonal incidence.
Virulence Diseases:
- Venereal syphilis (Treponema pallidum subspecies pallidum)
- Endemic syphilis or bejel (T. pallidum subspecies endemic:)
- Yaws (T. pallidum subspecies pertenue).
- Pinta (Treponema carateum)
Virulence Diagnosis:
- Treatment, Prevention, and Control
- Penicillin is the drug of choice; tetracycline, erythromycin, or chloramphenicol is administered if the patient is allergic to penicillin.
- Safe sex practices should be emphasized, and sexual partners of infected patients should be treated.
- Endemic syphilis, yaws, and pinta can be eliminated through organized public health measures (treatment, education); however, these efforts have been inconsistently applied.
Virulence Physiology and Structure:
- Epidemic relapsing fever – the etiologic agent is Borrelia recurrentis.
- Endemic relapsing fever – many Borrelia species are responsible.
- Lyme disease – Borrelia burgdorferi causes disease in the United States and Europe; Borrelia garinii and Borrelia afzelii cause disease in Europe and Asia.
- Spirochetes measure 0.2 x 0.5 to 30 pm can be seen when stained with aniline dyes (e.g., Giemsa, Wright stains).
- Can grow in culture, but bacteria are microaerophilic and have complex nutritional requirements.
Virulence factors:
- Borrelia responsible for relapsing fever are able to undergo antigenic shift and escape immune clearance; periodic febrile and febrile periods result from antigenic variation.
- Immune reactivity against Lyme disease agents may be responsible for the clinical disease.
Virulence Epidemiology:
- Epidemic relapsing fever: transmitted person-to-person; reservoir – humans; vector – human body louse.
- Endemic relapsing fever: transmitted rodents to humans; reservoirs – rodents, small mammals, and soft ticks; vector – soft ticks.
- Individuals at risk for relapsing fever include people exposed to lice (epidemic disease) in crowded or unsanitary conditions and people exposed to ticks (endemic disease) in rural areas.
- Epidemic relapsing fever is endemic in Ethiopia, Rwanda, and the Andean foothills.
- Endemic relapsing fever has worldwide distribution and is in the western states of the United States.
- Lyme disease: transmitted by hard ticks from mice to humans; reservoir – mice, deer, ticks; vectors include Ixodes scapularis in the eastern and Midwestern United States, Ixodes pacificus in the western United States, Ixodes ricinus in Europe, and Ixodes persulcatus in Eastern Europe and Asia.
- Individuals at risk for Lyme disease include people exposed to ticks in areas of high endemicity.
- Lyme disease has worldwide distribution.
- Seasonal incidence corresponds to the feeding patterns of vectors; most cases of Lyme disease in the United States occur in late spring and early summer (feeding pattern of nymphs).
Virulence Diseases:
- Epidemic relapsing fever.
- Endemic relapsing fever.
- Lyme disease.
Virulence Diagnosis:
- Either of the following:
- Erythema migrans (> 5 cm in diameter)
- At least one late manifestation (i.e., musculoskeletal, nervous system, or cardiovascular involvement) and laboratory confirmation of infection.
Virulence Laboratory criteria for diagnosis:
- At least one of the following: Isolation of Borrelia burgdorferi.
- Demonstration of diagnostic levels of IgM or IgG antibodies to the spirochetes.
- Significant increase in antibody titer between acute and convalescent serum samples.
- Treatment, Prevention and Control
- For relapsing fever, treatment is with tetracycline or erythromycin.
- For Lyme disease, treatment is with amoxicillin, tetracycline, cefuroxime, or ceftriaxone.
- Using insecticides and applying insect repellents to clothing can decrease exposure to the insect vector and wearing protective clothing that reduces exposure of skin to insects.
- The recombinant ospA vaccine is available for Lyme disease.
- Summary of Spirochetes
Virulence Differential Diagnosis Bacteria
- Between streptococci and staphyloma: Coagulase test: It is positive for staphylococci. Negative for streptococci.
- Lancefield grouping of streptococci: Presenceui carbohydrate.
- Between alpha-hemolytic and beta-hemolytic: Production of streptolysin ‘A’ and streptolysis ‘S’ by B-hemolytic bacteria.
- Between streptococci and staphyloma: Coagulase test: It is positive for staphylococci. Negative for streptococci.
- Lancefield grouping of streptococci: Presence carbohydrate.
- Between alpha-hemolytic and beta-hemolytic: Production of streptolysin ‘A’ and streptolysis ‘S’ by B-hemolytic bacteria.
- Between streptococci and staphyloma: Coagulase test: It is positive for staphylococci. Negative for streptococci.
- Lancefield grouping of streptococci: Presence carbohydrate.
- Between alpha-hemolytic and beta-hemolytic: Production of streptolysin ‘A’ and streptolysin ‘S’ by B-hemolytic bacteria.
Leave a Reply