Management Of Class 3 Malocclusion
Question 1. Classify etiology of malocclusion. Give the etiology and treatment of Angle’s Class 3 malocclusion.
Answer.
Class 3 Malocclusion
This malocclusion exhibit a class 3 molar relation with the mesiobuccal cusp of maxillary first permanent molar lies occluding in the interdental space between the mandibular 1st and 2nd molars.
Etiology of Angle’s Class 3 Malocclusion
Functional Factors
- Unfavorable anterior incisal guidance leads to class 3 malocclusion.
- If there is no treatment for functional cases, they become true class 3 malocclusion.
- Premature loss of deciduous molars can lead to mandibular displacement which leads to class 3 malocclusion.
- Loss of posterior teeth leads to loss of posterior proprioceptive support in habitual occlusion.
Read And Learn More: Orthodontics Question And Answers
“Understanding the role of orthodontics in managing Class 3 malocclusion: Q&A explained”
Soft Tissue Factors
- Flat anteriorly positioned tongue which lies low in mouth leads to class 3 malocclusion.
- Lack in eruption of posterior teeth because of the lateral tongue thrust leads to the overclosure of mandible. This leads to autorotation which causes class 3 malocclusion.
Hereditary Factors
They leads to skeletal or True Class 3 malocclusion.
Racial
Class 3 malocclusion is common in some races. e.g. Every individual in German Royal family has Habsburg jaw.
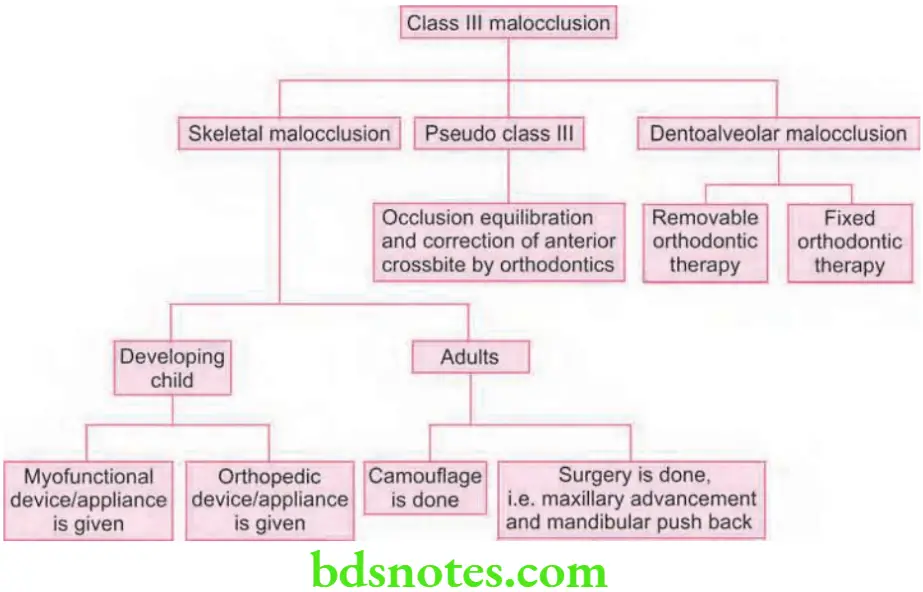
Treatment of Class 3 Malocclusion
Class 3 malocclusion should be recognized treated early due to:
- Severity of malocclusion can be decreased by intercepting abnormal skeletal growth pattern.
- Anterior crossbite results in retarded growth of maxilla due to locking of maxilla within the mandible.
- If not treated early mandible continues to grow forward and worsens prenormally.
“Importance of studying Class 3 malocclusion for better orthodontic outcomes: Questions explained”

Treatment of Class 3 Malocclusion
Objectives
- In skeletal cases growth modulation should be achieved.
- In relieving crowding and correction of alignment of teeth.
- Incisor relationship should be corrected.
- Anteroposterior as well as unilateral crossbite is corrected.
- Molar relationship should be stabilized.
“Common challenges in managing Class 3 malocclusion effectively: FAQs provided”
Skeletal Class 3 Malocclusion in Developing Child (Growing Child)
- In cases with midface deficiency in children functional appliances should be given in deciduous or mixed dentition.
- In functional appliances FR 3 is commonly used.
- In maxillary deficiency reverse pull headgears are indicated.
- In cases with prognathic mandible extraoral appliance like chin cup is advocated as early form of treatment.
- In cases with combined retrognathic maxilla and prognathic mandible reverse pull headgear or FR 3 with chin cup is used.
Treatment of Anterior Crossbite
Lower inclined plane or removable appliances incorporating the screws designed for the anterior expansion is used to treat mild anterior crossbite.
“Role of mandibular prognathism in Class 3 malocclusion: Questions answered”
Treatment of Posterior Crossbite
It is treated by rapid maxillary expansion.
Role of Extractions
- Class 3 malocclusion is characterized by lower arch length deficiency and anterior crossbite can be treated by extracting mandibular fist premolars followed by fixed appliances
- First premolars should be extracted in both maxillary and mandibular arches, in case of arch length deficiency both the arches are involved.
“Why is proper management critical for Class 3 malocclusion success? Answered”
Skeletal Class 3 Malocclusion in an Adult (After Growth)
- Camouflage is attempted in mild skeletal class 3 cases.
- For achieving good occlusion mandibular premolars should be extracted and class 3 elastics and chin cup is given.
- In camouflage retraction of mandibular molars makes chin prominent which is a drawback.
- In class 3 camouflage extraction of maxillary second premolars and mandibular fist premolar can be done which is followed by class 3 intermaxillary elastics which causes mandibular incisor retraction as well as molar correction.
- Surgical management can be done by maxillary advancement and by mandible push back.
- Sometimes a combination of upper and lower jaw surgery is done with reduction genioplasty.
Treatment of Pseudo Class 3/Function Class 3/Postural Class 3
- In early treatment occlusal equilibration is carried out.
- In late treatment correction of anterior crossbite is done.
Dentoalveolar Correction
- If one or two incisors are in crossbite removable appliances are used. Appliances used as anterior expansion plate and Z spring.
- Fixed appliances can also be used. Cases are treated either by extraction or non-extraction.
“Steps to explain different types of Class 3 malocclusion: Skeletal vs dental: Q&A guide”
Question 2. How will you manage a case of developing class 3 malocclusion.
Answer.
Management of a Case of Developing Class 3 Malocclusion
Leave a Reply