Malignant Tumors Of Jaws Question And Answers
Question 1. Write short note on malignant melanoma of Oral Cavity.
Answer. Malignant melanoma is the neoplasm of epidermal melanocytes.
Malignant melanoma is the biologically unpredictable and is deadly of all the human neoplasms.
Oral Cavity Etiology
- Sunlight: For cutaneous melanoma sunlight is most important factor. Acute sun damage leads to be more destructive as compared to chronic sun damage.
- Genetic: Chances of malignant melanoma is more in person in whom family malignant melanoma was detected.
- Other factors: Patient’s having fair complexion, history of blistering sunburns, history of nevus can undergo malignant melanoma.
“Importance of studying jaw tumors for better diagnostic outcomes: Questions explained”
“Understanding malignant jaw tumors through FAQs: Q&A explained”
Types malignant melanoma of oral cavity
- Superficial spreading melanoma: Most commonly occurring type
- Nodular melanoma: This is the form of cutaneous melanoma and occurs mainly in head and neck region.
- Lentigo maligna melanoma: It develops from precursor lesion such as lentigo maligna.
- Acral lentiginous melanoma: This is most common type in blacks and occurs commonly in oral cavity.
Growth Pattern of Oral Cavity
- Radial growth: It last for several months to years. During radial growth malignant melanocytes spread horizontally via basal layer of epidermis.
- Vertical growth: It is characterized by increase in size, change in the color, nodularity and at times the ulceration. Here malignant cells invade connective tissue.
Read And Learn More: Oral Medicine Question And Answers
Malignant Melanoma of Oral Cavity Clinical Features
Superficial Spreading Melanoma of Oral Cavity
- It occurs during 5th to 7th decades of life. More common in males as compared to females.
- It occurs as tan brown, black or admixed lesion over the sun exposed skin mainly in blacks.
- It can also involve skin of face, head and neck, chest, abdomen and the extremities.
- It initially begins as pigmented macule which shows superficial radial growth pattern and is restricted to epithelium as well as junction. In advanced cases, it is ulcerated shows fungating growth and is associated with bleeding.
Nodular Melanoma of Oral Cavity
- It occurs in head and neck, and is more common in males.
- It is mucosal pink to brown and blue to black in color.
- It is firm on palpation.
- It consists of erythematous borders which surround the tumor.
- It can ulcerate and hemorrhage can be seen. In later stage, it is more diffuse, nodular and tumefactive having foci of hypopigmentation and hyperpigmentation.
- This is presented as sharply delineated nodule along with some degree of pigmentation.
“Common challenges in diagnosing malignant jaw tumors effectively: FAQs provided”
Lentigo Maligna Melanoma
- It is more common in females and occurs more commonly in the exposed parts.
- It presents as pigmented macule along with ill defined margins.
- It shows radial growth with around central axis and in the superficial manner.
- In later stages, it shows invasion and metastasis.
Acral Lentiginous Melanoma
- It occurs on palm of hands, sole of feet, sublingual area and the mucous membrane.
- It develops as dark pigmented irregularly marginated macule.
Jaw Malignancy: Key Questions and Management
Oral Cavity Oral manifestations
- It is uncommon in oral cavity and occurs more commonly in man at the age of 40 to 70 years with mean age of 55 years.
- It has predilection for palate, maxillary gingiva/alveolar gingiva which is followed by buccal mucosa, tongue, lip and floor of the mouth.
- Oral melanomas are painless. Lesion is soft, darkish brown or black mass. It consists of either nodular or papillary surface.
- Lesion appears as deeply pigmented, sometimes ulcerated and hemorrhagic and increase progressively in size.
- Tumor leads to destruction of the underlying bone with loosening of teeth.
Oral Cancer: Malignant Tumors of the Jaws and Their Treatment
Malignant Melanoma of Oral Cavity Diagnosis
- Clinical diagnosis: Presence of darkly pigmented lesion along with the ulceration.
- Laboratory diagnosis: In superficial spreading melanoma, melanocytes are arranged in “pagetoid manner”. In nodular melanoma, large epithelioid melanocytes under the connective tissue are present. Lentigo melanoma consists of increased number of atypical melanocytes with basal epithelial layer.
Malignant Melanoma of Oral Cavity Management
- Surgical removal of lesion along with the removal of regional lymph nodes.
- Other therapy: Irradiation, immunotherapy and chemotherapy or combination can be tried.
“Why is early detection critical for managing jaw malignancies? Answered”
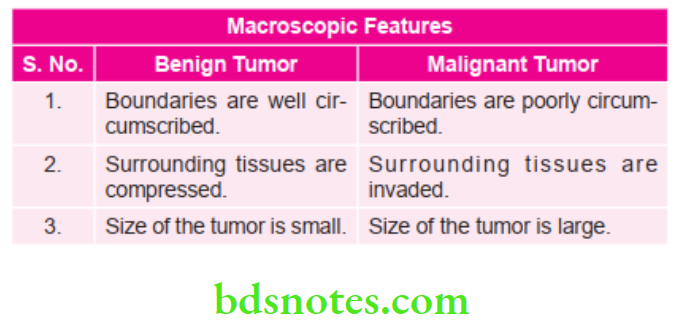
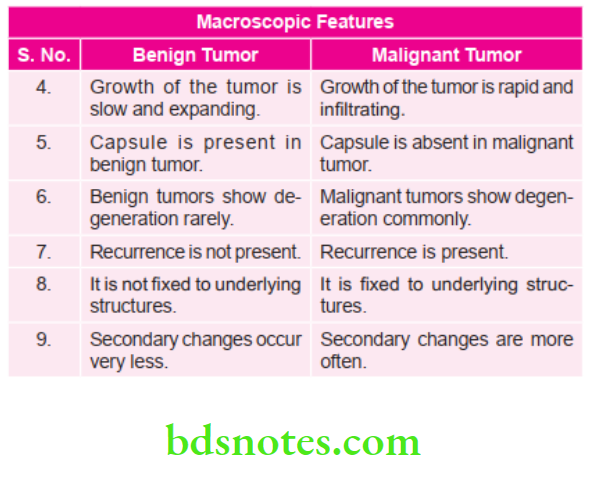
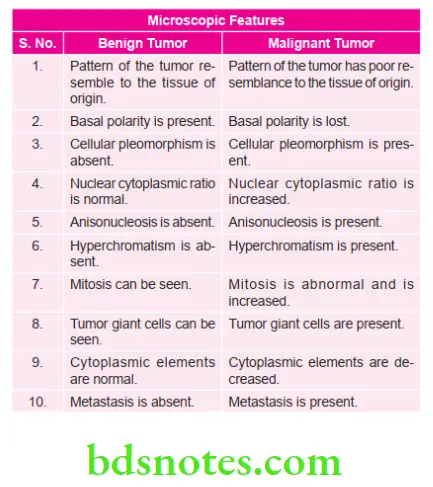
Question 2. Write short note on difference between benign and malignant tumors.
Answer.
“Factors influencing success with jaw tumor treatment: Q&A”
Question 3. Write short note on Radiation Mucositis.
Answer. It is the inflammation of oral mucus membrane following radiotherapy.
- The basal layer of oral mucous membrane contains differentiating inter mitotic cells. These cells are sensitive to radiation.
- It develops in second week of radiotherapy.
- There are areas of redness and inflammation.
- Later on mucus membrane brakes down to form pseudomembrane.
- After some period mucus membrane becomes atrophic and thick.
- It is managed with the application of topical anesthetic agents for relief of pain, most commonly used is doxycycline hydrochloride.
“Steps to explain causes of malignant jaw tumors: Radiation vs genetic mutations: Q&A guide”
Question 4. Describe the radiographic appearance of osteosarcoma.
Or
Write short note on radiographic features of osteosarcoma.
Or
Write radiographic appearance of osteogenic sarcoma of jaw.
Or
Write short note on radiographic features of osteogenic sarcoma
Answer. Osteosarcoma as per the radiographic appearance is divided into 3 stages.
- Osteolytic stage
- During this stage, radiograph show moth eaten appearance.
- In osteosarcoma, the borders are ill defined and margins are unicentric.
- The cortical plates are perforated and show expansion.
- Pathological fractures are seen.
- Neurovascular canal is widened.
- Resorption of the teeth roots is seen of the involved area.
- Tumor may grow with in periodontal membrane space causing resorption of adjacent bone leading to widening of periodontal membrane space.
- Mixed Stage:
- Duringthis stage, radiograph shows honey comb appearance.
- Margins of lesion are not well defined.
- Presence of bone formation as well as bone destruction is evident on radiograph.
- At times, bone is seen which is present inside the tumor.
- If tumor involves the maxillary sinus and nasal fossa, then they are invaginated.
- Osteoblastic Stage
- During this stage, radiograph shows onion-peel appearance.
- Alveolar ridge is distorted.
- Attimes, radiograph shows granular or sclerotic appearance.
- Small streaks of bone radiate outward which produces a Sun-ray appearance.
- In long bones affected with osteosarcoma, periosteum is elevated over the expanding tumor mass in a tent-like fashion. At the point, on the bone where periosteum begins to merge an acute angle between bone surface and periosteum is created. This is called as Codman’s triangle.
“Role of carcinogens in causing jaw malignancies: Questions answered”
Question 5. Write short note staging and grading of oral cancer.
Answer.
- Staging of oral cancer is done by TNM classification.
- TNM classification was given by American Joint Committee on Carcinoma (AJCC)
- T is suggestive of Primary tumor
- N is suggestive of Regional lymph nodes
- M is suggestive of Distant metastasis
- T – Primary tumor.
- TX – Primary tumor cannot be assessed.
- T0 – No evidence of primary tumor.
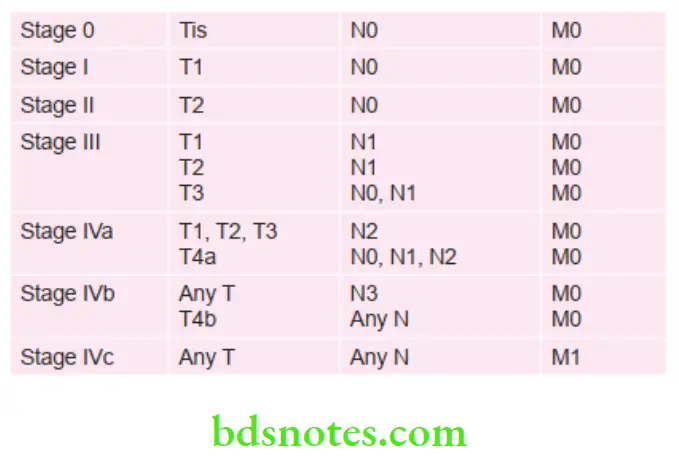
- Tis – Carcinoma in situ.
- T1 – Tumor 2 cm of less in greatest dimension.
- T2 – Tumor more than 2 cm but not more than 4 cm in greatest dimension.
- T3 – Tumor more than 4 cm in greatest dimension.
- T4a (Lip) – Tumor invades through cortical bone, inferior alveolar nerve, floor of mouth or skin (chin or nose).
- T4a (Oral Cavity) – Tumor invades through cortical bone, into deep/extrinsic muscle of tongue (genioglossus, hyoglossus, palatoglossus and styloglossus), maxillary sinus or skin of face.
- T4b (lip and oral cavity) – Tumor invades masticatory space, pterygoid plates or skull base or encases internal carotid artery.
- N – Regional lymph nodes.
- NX – Regional lymph nodes cannot be assessed.
- N0 – No regional lymph node metastasis.
- N1 – Metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension.
- N2a – Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension.
- N2b – Metastasis in multiple ipsilateral lymph nodes, not more than 6 cm in greatest dimension.
- N2c – Metastasis in bilateral or contralateral lymph nodes, not more than 6 cm in greatest dimension.
- N3 – Metastasis in a lymph node more than 6 cm in greatest dimension.
- M – Distant metastasis.
- MX – Distant metastasis cannot be assessed.
- M1 – No distant metastasis.
- M2 – Distant metastasis is present.
“How does bone invasion occur in malignant jaw tumors? FAQ explained”
Staging Of Oral Cancer
Grading of Oral Cancer
Grading is defined as macroscopic and microscopic degree of differentiation of tumor.
Broader’s Grading of Oral Cancer
- Grade 1: Well differentiated (< 25% anaplastic cells)
- Grade 2: Moderately differentiated 25–50%
- Grade 3: Moderately differentiated 50–70%
- Grade 4: Poorly differentiated or anaplastic (More than 75% Anaplastic cell).
“Early warning signs of issues addressed by understanding jaw tumor pathogenesis: Common questions”
Question 6. Write short note on management of oral squamous cell carcinoma.
Or
Write short note on treatment of oral cancer.
Answer. Oral cancer is treated by surgery, radiotherapy and chemotherapy or by combination of these.
The other developing techniques in the treatment of oral cancer are laser therapy, hormonal therapy, hyperthermia, etc.
Surgery oral cancer
1. The surgical treatment of oral cancer as a primary modality is excisional in nature.
2. All clinical detectable tumor must be excised with adequate margins of adjacent normal tissue, to ensure that the residual element of the microscopic disease do not remain within the surgical field.
3. Surgical treatment has two distinctive phases, i.e. resection of the tumor and the reconstruction of the defect.
Different types of surgeries may be performed.
Curettage oral cancer
- In curettage hand instruments are used for the removal.
- During curettage, margin of normal bone is removed for ensuring that there is complete removal of tumor.
- As lesion is removed, sharp bony spicules are rounded by bur or rougeur.
- Primary closure of small boney lesions is done.
- Large lesions are closed by secondary intention
En bloc Resection oral cancer
- It is removal of the entire tumor along with adequate margins of surrounding normal tissue.
- Localized tumor without suspected cervical lymphatic involvement is treated by this method.
Mandibular Segmental Resection oral cancer
Following is the procedure:
- Anterior to the lesion a bony cut is given which extend to inferior border of mandible by Gigli saw or bur.
- As cut is made lateral rotation of segment is done, while entering mandibular foramen, inferior alveolar bundle is ligated.
- Condyle is now free off from lateral pterygoid muscle and disarticulation of mandible is done.
- Hemostasis is attained and closure of flaps is accomplished.
- Drain is placed over the dead space for collection of fluid.
“Asymptomatic vs symptomatic effects of ignoring jaw tumor triggers: Q&A”
Reconstruction of mandible oral cancer
In reconstruction of mandible, simple reconstruction plate is used, free bone grafts are given.
Maxillectomy oral cancer
In tumors involving the maxilla, partial or total maxillectomy is done depending on extension of the tumor.
Radiotherapy: oral cancer oral cancer
Radiotherapy is the treatment of the disease with ionizing or non-ionizing radiation.
Following methods are to be followed for radiotherapy
- X-ray therapy
- Superficial X-ray therapy 45–100 kV
- Kilovoltage X-ray therapy 300 kV
- Electron therapy
- Surface applicator
- Interstitial implantation:
- Radiation is given externally by the use of X-ray generators.
- Uninvolved areas of patient should be prevented by doing shielding.
- Host tissues of patient should be protected from radiation by two methods, i.e. fractionation and multiple ports.
- In fractionation instead of giving maximum radiation patient is given radiation in small increments for several weeks which provides time for normal tissues for recovery between dosages.
- In multiple ports, multiple beams are used which provide radiation to tumor from different angles. In this, radiation delivery is on every 5th day a week.
Chemotherapy
- It is used in the treatment of malignant tumor. It selectively Kill’s tumor cells by virtue of cell kinetic proliferation character and cell biology.
- Chemicals which interferes with rapid growth of tumor cells are used for treating oral cancer.
- Vincristine, bleomycin and methotrexate in various combinations are used.
- Chemotherapy should be given intravenously but nowadays, it intra-arterial injections can be given
- It produces only partial or temporary tumor regression.
- It may be used in combination with radiotherapy or surgery or as palliative treatment.
- Chemotherapy is most effective in the lesions which are confined to the soft tissues.
“Steps to understand complications of jaw tumors: Fractures vs nerve damage: Q&A guide”
Question 7. Write short note on etiology and investigations of oral cancer.
Answer. For etiology in detail refer to Ans 2 of same chapter.
Investigations of Oral Cancer
In routine practice, the diagnostic tests implicated are:
- Vital staining: Toluidine blue is used to assess the oral cancer. Toluidine blue is a metachromatic dye which binds with DNA. The dye can be applied directly to suspicious lesions or can be used as an oral rinse. Positive retention of dye occurs in peripheral pattern of carcinomatous ulcer. This indicates need for biopsy.
- Brush biopsy: Here the cytobrush is combined with the computer assisted analysis of cytologic sample, assessing cell morphology and keratinization. Final diagnosis was mad by an oral pathologist based on standard histomorphologic criteria.
- Exfoliative cytology: Here tissue is acquired for histopathology by using fine needle aspiration or core needle biopsy. This aids in evaluation of suspected masses in other areas of head and neck.
- Tissue biopsy: In this technique, a portion of lesion is cut for the histopathological examination. It is a golden standard.
- Imaging techniques: Routine radiography, CT, MRI, nuclear scintiscanning and ultrasonography provides evidence of bone involvement or indicate the extent of some soft tissue lesions.
- For the early diagnosis of an oral malignancy new diagnostic tools such as VELscope and Vizilite plus, spectroscopy, high performance laser spectroscopy—laser-induced fluorescence play an important role.
- VELscope leads to the direct visualization of tissue fluorescence. Handpiece of the device emits the blue light in oral cavity leading to tissue fluorescence from surface of epithelium via basement membrane where premalignant changes start.
- As Vizilite plus passes over the oral tissue treated by rinsing solution, normal healthy tissue will absorb the light and appear dark while abnormal tissue appear white.
“Can targeted interventions improve outcomes using knowledge of etiology? Answer provided”
Question 8. Name Premalignant Lesions. Describe etiology, clinical and Radiographic Features, Treatment modalities of oral cancer.
Answer. Premalignant lesion is defined as a morphologically altered tissue in which cancer is more likely to occur than its apparently normal counterparts. WHO (1972)
For example,
- Leukoplakia
- Erythroplakia
- Mucosal changes associated with smoking habits
- Carcinoma in situ
- Bowen disease
- Actinic keratosis, actinic chelitis and actinic elastosis
Leave a Reply