Gingival Hyperplasia
Question. Classify gingival hyperplasia and describe leukemia.
Answer.
Classifiation of Gingival Hyperplasia
On basis of etiological factors and pathologic changes
- Inflammatory enlargement
- Chronic
- Acute
- Drug-Induced Enlargement
- Enlargement associated with systemic disease
- Conditional enlargement
- Pregnancy
- Puberty
- Vitamin C deficiency
- Plasma cell gingivitis
- Non-specifi conditioned enlargement (Pyogenic granuloma)
- Systemic diseases causing gingival enlargement
- Leukemia
- Granulomatous disease (E.g. Wegner’s Granulo matosis, sarcoidosis)
- Conditional enlargement
- Neoplastic Enlargement
- Benign tumors
- Malignant tumors.
- False Enlargement.
gingival hyperplasia
“Role of medications in causing gingival hyperplasia”
Using the criteria of location and distribution gingival enlargement is designated as follows:
- Localized: Gingival enlargement limited to one or more teeth.
- Generalized: Involving the gingiva throughout the mouth.
- Marginal: Confied to marginal gingiva.
- Papillary: Confied to interdental papilla.
- Diffse: Involving the marginal and attched papillae.
- Discrete: Isolated sessile or pedunculated tumor like enlargement.
On basis of degree of gingival enlargement
Grade 0: No sign of gingival enlargement.
Grade I: Enlargement confimed to interdental papilla.
Grade II: Enlargement involves papilla and marginal gingiva.
Grade III: Enlargement covers three quarters or more of the crown.
causes of gingival hyperplasia
“Can phenytoin cause gum overgrowth?”
Leukemia
Leukemia is a disease which is characterized by overproduction of
WBCs which are present in circulating blood in an immature form.
Types of Leukemia
- Acute
- Chronic
Etiology
- Chromosomal abnormality: Presence of an abnormal chromosome, e.g. Philadelphia chromosome.
- Exposure to high doses of radiation therapy.
- Exposure to certain chemicals, e.g. phenyl butazone and benzene.
- Myeloproliferative disorders like polycythemia vera.
- Congenital or genetic abnormalities.
- Presence of primary immune defiiency
- Infection with human leukocyte virus.
“Impact of cyclosporine on gingival hyperplasia”
Acute Leukemia
Classification of Acute Leukemia (FAB Classifiation)
1. Acute myeloblastic leukemia (AMD)
- M0: Minimally differentiated: Myeloblasts lack defiite cytologic and cytochemical features but have myeloid lineage antigens.
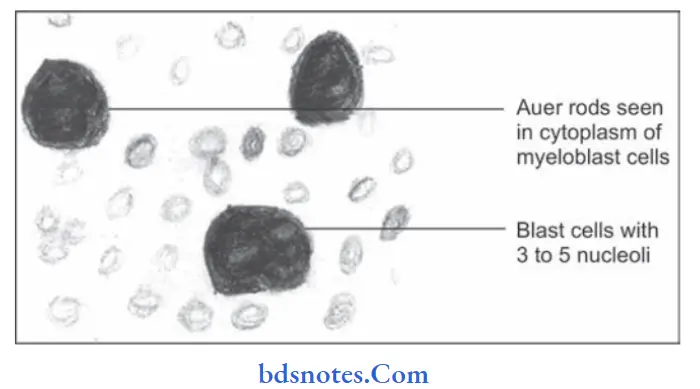
- M1: AML without maturation: Myeloblasts
predominate with distant nucleoli, few granules or Auer rods are present. - M2: AML with maturation: Myeloblasts with promyelocytes predominate and Auer rods may be present.
- M3: Acute promyelocytic leukemia: Hypergranular promyelocytes often with multiple Auer rods are seen.
- M4: Acute myelomonocytic leukemia: Mature cells of both myeloid and monocytic series in peripheral blood; myeloid cells resemble M2
- M5: Acute monocytic leukemia: Promonocytes or undiffrentiated blast.
- M6: Acute erythroleukemia: Erythroblast predominate;myeloblasts and promyelocytes also increased
- M7: Acute megakaryocytic leukemia: Pleomorphic undiffrentiated blast cells predominate and react with antiplatelet antibodies.
2. Acute lymphoblastic leukemia
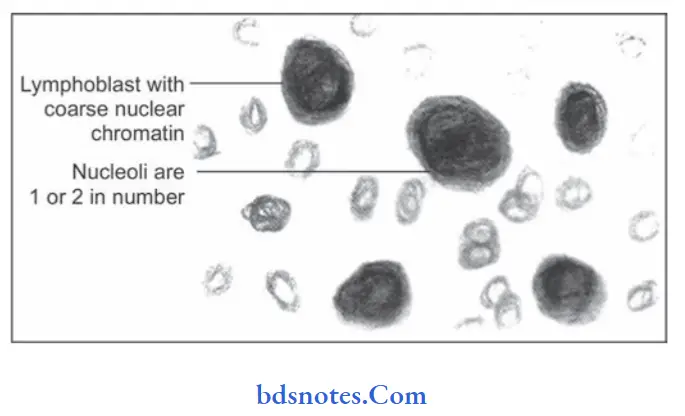
- L1: Acute lymphoblastic (Seen in children): Homogeneous small lymphoblasts; scanty cytoplasm,regular round nuclei, inconspicuous nucleoli.
- L2: Acute lymphoblastic (Seen in adults): Heterogeneous lymphoblasts; variable amount of
cytoplasm, irregular or cleft nuclei, large nucleoli. - L3: Burkitts type (Uncommon): Large homogenus lymphoblasts; nuclei are round to oval, prominent nucleoli, cytoplasmic vacuolation.
“Genetic factors leading to gingival hyperplasia”
Clinical Features
Acute leukemias are more common in children and adults from 1st to 4th decades of life.
Clinical features are due to:
- Bone marrow failure
- Anemia is seen leading to pallor, lethargy and dyspnea.
- Pyrexia is present.
- Bleeding manifestations are present, such as spontaneous bruises, petechiae, bleeding from gingiva.
- Infections of multiple organs are present.
- Organ infiltration
- Presence of pain and tenderness in bones.
- Enlargement of tonsils is present.
- Lymphadenopathy is seen.
- Hepatomegaly and splenomegaly are common findings.
- Chloroma or granulocytic sarcoma is a localized tumor mass occurring over the skin or orbit by local infiltration of tissues by leukemic cells.
“Symptoms of gingival hyperplasia”
Oral Manifestations
- Bleeding from gingiva is present. Gingiva becomes boggy,edematous and red in color.
- Presence of paresthesia of lower lip.
- Crustation over lips is seen.
- Mobility of permanent teeth is present.
- Oral mucosa appears pale with ulceration along with petechiae and ecchymosis.
Laboratory Findings
- Anemia: It is normochromic in type, moderate reticulocytes are seen, few nucleated red cells.
- Thrombocytopenia: Platelet count is below 50,000/µl of blood.
- WBC count: It ranges from subnormal to markedly elevated. It is 1,00,000/µl of blood in advanced cases. Leucocytes in peripheral blood are blast cells.
- Bone marrow examination shows hypercellularity. Bone marrow is packed with leukemic blast cells. Erythropoietic cells are reduced. Megaloblastic features and ring sideroblasts are present.
“Signs of gum overgrowth in adults”
Chronic leukemia
These are hematologic malignancies in which predominant leukemic cells are initially well differentiated. They are of two
types:
1. Chronic myeloid leukemia
2. Chronic lymphocytic leukemia
“Red flags of severe gingival hyperplasia”
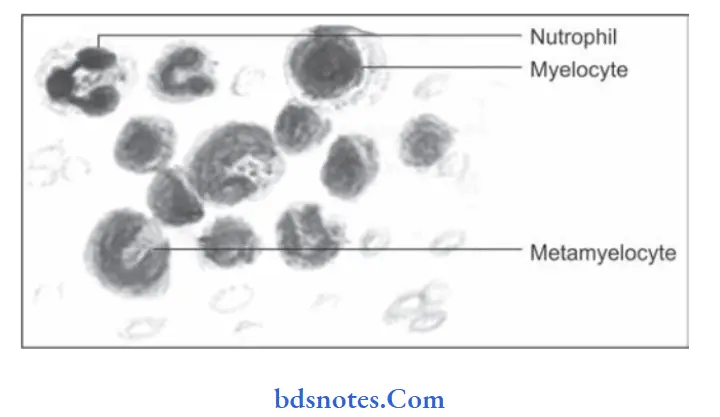
Chronic myeloid leukemia
It consists of large leukemic cells and diffrentiated WBCs in bone marrow.
Clinical Features
- It occurs during 3rd and 4th decades of life.
- Splenomegaly is present.
- Patient complains of loss of weight, abdomen prominence.
- Presence of anemia leads to weakness, fatigue and dyspnea.
- Petechiae and ecchymosis is seen.
“Pain and discomfort in gingival hyperplasia”
Laboratory Findings
- Anemia is normocytic and normochromic type.
- Marked leucocytosis is present, i.e. 2,00,000 cells/µl.
- There is increased proportion of basophils.
- Bone marrow shows hypercellularity with total or partial replacement of fat spaces by proliferating myeloid cells.
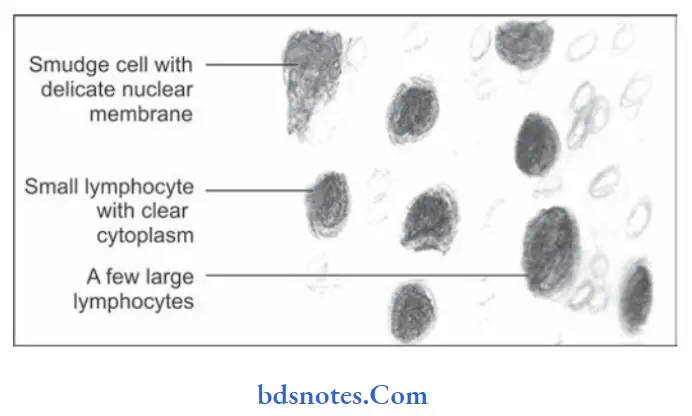
Chronic lymphocytic leukemia
It is the malignancy of mature B cells.
Clinical Features
- It occurs during 4th decade of life.
- Male predilection is seen.
- Features of anemia are seen, i.e. weakness, fatigue and dyspnea.
- Lymphadenopathy is commonly present.
- Hepatomegaly and splenomegaly is commonly seen.
- Hemorrhagic manifestations are common.
“Bleeding gums and gingival hyperplasia”
Oral Manifestations
- Gingival hypertrophy is present. Ulceration of gingiva with necrosis is present.
- Tongue is dark and swollen.
- Presence of mobility of teeth is seen.
- Necrosis of PDL is seen.
- Alveolar bone destruction is also present.
Laboratory Findings
- Anemia is mild to moderate and is normocytic normochromic type.
- Marked leucocytosis is present.
- Leucocytes are mature small lymphocytes.
- Platelet count is normal or moderately reduced.
“Surgical removal of excess gum tissue”
Treatment
Chemotherapeutic drugs, radiation therapy and corticosteroids which leads to prolong remission and cures in some forms of disease.
Leave a Reply