Different Types Of Mandibular Fractures
Types Of Mandibular Fracture
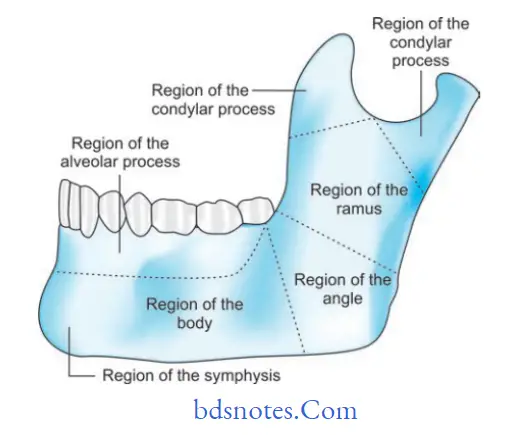
Dingman and Natvig Anatomic Classification
- Midline: Fractures between central incisors.
- Symphysis: Fractures occurring within the area of symphysis.
- Parasymphysis: Bounded by vertical lines distal to canine teeth.
- Body: From distal symphysis to a line coinciding with the alveolar border of the masseter muscle usually including the third molar.
- Angle: Triangular region bounded by the anterior border of the masseter muscle to posterosuperior attachment of the masseter muscle.
- Ramus: Bounded by the superior aspect of the angle to two lines forming an apex at the sigmoid notch.
- Condylar process: Area of condylar process superior to the ramus region.
- Coronoid process: Includes coronoid process ofthe mandible superior to the ramus region.
- Dentoalveolar process: Region that would normally contain the teeth
Mandibular Fracture Types
Read And Learn More: Maxillofacial Fractures, Disorders, and Treatments
“Can Braces Help After A Mandibular Fracture“
Condylar Mandibular Fracture
Mandibular Fracture Clinical Presentation/ Clinical Features
Fracture at angle
- Swelling at the angle externally and there may be obvious deformity.
- Laceration of skin or mucosa.
- Step deformity behind the last molar tooth may be visible which is more apparent if no teeth are present in the molar region.
- Undisplaced fractures are usually revealed by the presence of a small hematoma adjacent to the angle on either the lingual or buccal side, or both.
- Anesthesia or paraesthesia of the lower lip may present on the side of the fracture.
- Inability to close the jaw causing premature dental contact.
- Occlusion is often deranged. Movements of the mandible are painful and the range of movements is reduced.
- Trismus to some degree is usually present.
- Anterior open bite is seen in bilateral angle fracture.
- Ipsilateral open bite is seen in unilateral ankle fracture.
Body Mandibular Fracture
“Best Practices For Post-Surgical Care Of Mandibular Fractures“

Ramus Mandibular Fracture
Mandibular Fracture of the Body
- Physical signs and symptoms such as swelling and bone tenderness are similar to those seen in the fracture of the angle of the mandible.
- Even slight displacement of the fracture causes derangement of the occlusion.
- Premature contact occurs on the distal fragment because of the displacing action of muscles attached to the ramus.
- Fractures between adjacent teeth tend to cause gingival tears.
- When there is gross displacement, the inferior dental artery may be torn, and this can give rise to severe intraoral hemorrhage.
- Sublingual hematoma or ecchymosis in the floor of the mouth.
- The flattened appearance of the lateral aspect of the face.
- Inability to open or close the jaw.
- Crepitation on palpation.
“Effective Ways To Manage Mandibular Fracture Recovery”
Alveolar Mandibular Fracture
Fracture of Symphysis and Parasymphysis
- These fractures are commonly associated with fractures of one or both condyles.
- This fracture may be missed if occlusion is undisturbed locally.
- The presence of bone tenderness and a small lingual hematoma may be the only physical signs.
- Sublingual hematoma or ecchymosis in the floor of the mouth.
- Posterior open bite or unilateral open bite is seen in para-symphysis fracture. Posterior crossbite can result from midline symphysis fractures.
- Crepitation on palpation is noted in a symphyseal fracture.
- An inability to close the jaw causes premature dental contact.
- A retruded chin can be caused by a bilateral parasymphyseal fracture.
- The fracture line is often oblique, which allows over-riding of the fragments with lingual inversion of the occlusion on each side.
Fracture Of Ramus
- They are uncommon.
- The flattened appearance of the lateral aspect of the face.
- Inability to open or close the jaw.
- Swelling and ecchymosis are usually noted both extraorally and intraorally.
- Tenderness over the ramus and movements produce pain over the same area.
- Severe trismus is present.
- Fracture of the Coronoid Process
- The fracture can be caused by direct trauma to the ramus, but it is rarely isolated. It is usually considered to result from the reflex contracture of the powerful anterior fibers of the temporalis muscle.
- This fracture is difficult to diagnose clinically.
- Tenderness over the anterior part of the ramus.
- Painful limitation of movement, especially during protrusion of the mandible, may be found.
- It depends on the line of fracture.
- An oblique fracture shows a bad prognosis.
- Spiral fracture shows a good prognosis due to increased surface area.
“The Role Of Imaging In Diagnosing Mandibular Fractures”
Mandibular Fracture Classification
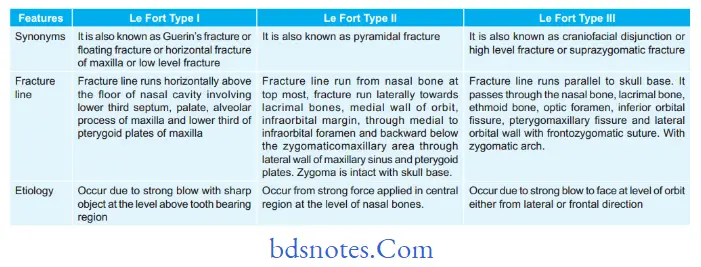
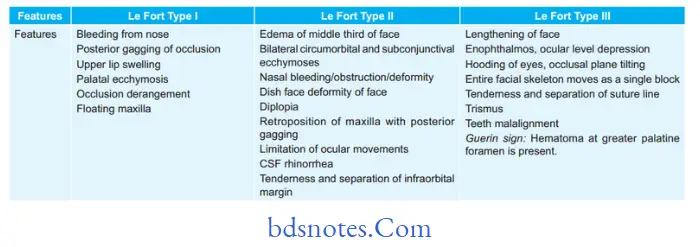
Question 2. Describe differentiating features of Le Fort Type I, II, and III fractures
Answer.
Differentiating Features Of Le Fort Type I,Ii, And Iii Fractures In Table
Parasymphysis Mandibular Fracture
“Comprehensive Overview Of Mandibular Fracture Types“
Leave a Reply