Epidemiology, Etiology, And Prevention Of Dental Caries
Question 1. Write a short note on the caries-prone area.
Answer. Caries-prone area refers to the area in which dental caries is most likely to occur.
- Dental caries is higher in the maxillary arch.
- Permanent molars have incompletely coalesced pits and fissures that allow dental plaque material to be retained at the base of a defect in contact with exposed dentin.
- Palatal pits of maxillary molars, buccal pits of mandibular molars, and palatal pits on maxillary incisor teeth are more prone than their maxillary counterparts.
- The second molar is more prone to caries than 1st molar.
- The distal surface of the deciduous 2nd molar is most prone to the permanent molar.
- Deciduous maxillary incisors are more susceptible to nursing bottle caries.
“Understanding dental caries: Prevention techniques explained”
“Importance of early intervention in dental caries prevention”
Question 2. Discuss the epidemiology of dental caries in our country.
Answer. In India, there is evidence of an increasing caries rate in children and adults.
- Dental caries has been consistently increasing both in prevalence and severity since the last 5 decades.
- In India, data from the National Oral Health Survey (2002–03) states that in children aged 12 years, caries prevalence was 53.8% and mean DMFT was 1.8, whereas it was 80.2% and 5.4 in the 35–44 year age group. In the 65–74 year age group, the prevalence was 85% and the mean DMFT was 14.9.
- WHO reported a DMFT score of 3.94 for India in 2003.
- The relationship between increased industrialization, consumerism, consumption of refined carbohydrates and sugars, and caries rates is well known with increasing urbanization.
- People are switching from traditional starchy staple foods to refined carbohydrates.
- The caries rate in India also depends on the individual’s current socioeconomic status.
- The sophistication and development of dental services depend on access and availability of dentists.
- In rural areas dental care if available consists of palliative services and extraction, while replacement of lost teeth with a prosthesis is exceptional.
- Populations in urban areas have the greatest access to care, but the quality and sophistication of care depend on the socioeconomic status of the individual seeking care.
- In India there is need to develop national preventive programs to combat the rising caries rate. These preventive programs must not only present known scientific facts, but also confront the deep seated beliefs of the people that have been handed down from folklore.
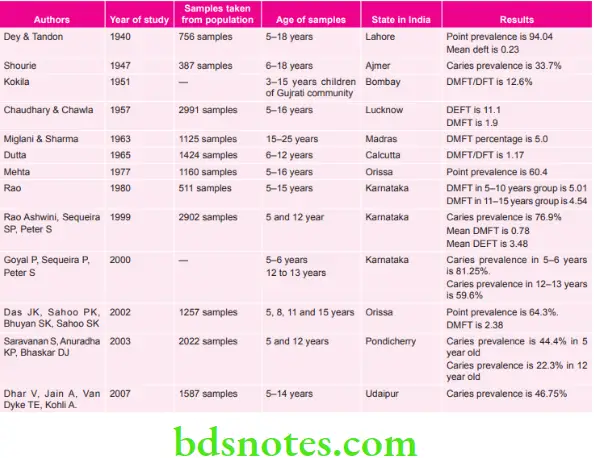
- Tabulation of data from various studies regarding the epidemiology of dental caries, which were done in India, is:
“Common causes of dental caries and how to prevent them”
“Signs that fluoride prevents dental caries effectively”
Question 3. Write briefly on the risk factors of periodontal diseases and dental caries.
Answer. Epidemiology, Etiology, and Prevention of Periodontal Disease.
Risk Factors of Dental Caries
- Medium or high S. mutans and Lactobacillus counts.
- Visible heavy plaque on teeth: This indicates poor oral hygiene and/or prolific plaque growth by the individual and is an indirect indicator that there are likely to be high levels of cariogenic bacteria.
- Inadequate exposure to fluoride
- Frequent (>three times daily) snacking between meals: lf a person is snacking greater than 3 times daily between meals on foods or beverages that contain sucrose, glucose, fructose, or cooked starch (cookies or bread) this increases the acid challenge to the teeth to a high level.
- Deep pits and fissures
- Lower socioeconomic status
- Recreational drug use
- Inadequate saliva flow by observation or measurement: Saliva reducing factors (medications/radiation/systemic). Saliva flow rate can be measured by having the patient chew and spit into a measuring cup and calculating the number of milliliters (mL) per minute. A value less than 0.7 mL/minute is low, whereas 1–4 mL/minute is normal.
- Exposed roots
- Orthodontic appliances: Presence of fixed or removable appliances in the mouth such as orthodontic brackets or removable partial dentures leads to undue accumulation of plaque and an increase in the percent of cariogenic bacteria. These appliances will generally place the patient at high risk of new carious lesion in the future.
- Any physical or mental illness and any oral application or restoration that compromises the maintenance of optimal oral health.
Read And Learn More: Public Health Dentistry Question And Answers
“Role of fluoride varnish in preventing tooth decay”
Question 4. Write a short note on the Vipeholm study.
Answer. The Vipeholm study was given by Gustaffson et al (1954), and it was summarized by Davies (1955).The
- Vipeholm study was an investigation of five years carried out on 436 adults in Vipeholm hospital in Lund, Sweden.
- Vipeholm Hospital was an institution for mentally challenged individuals.
Purpose of Study
To rule out the answers to some questions, i.e.
Does an increase in carbohydrate intake cause an increase in dental caries?
If it is so, then caries is actively influenced by
- Ingestion at meals of refined sugar in non-sticky form.
- Ingestion at meals of sugar in sticky form
- Ingestion of sugar between meals in a sticky form.
Does a decrease in carbohydrate intake cause a decrease in dental caries?
Vipeholm Study Method of Study
- The diet of the institution was nutritious and consisted of a little sugar with no provision for between-meal snacks.
- Daily, four meals were taken.
- The rate of dental caries in inmates is low.
- Design of the study divides inmates into one control and six experimental groups:
“Biomechanics of fluoride’s role in enamel remineralization”
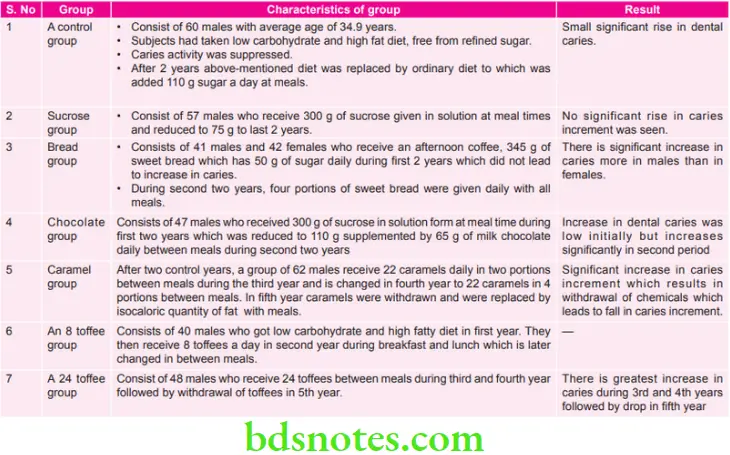
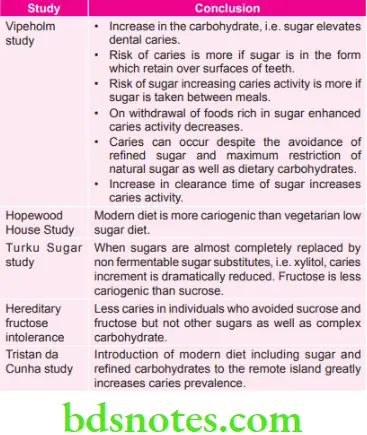
Vipeholm Study Conclusion
- An increase in the carbohydrate, i.e., sugar, elevates dental The risk of caries is higher if sugar is in the form that remains on the surfaces of teeth.
- The risk of sugar increasing caries activity is higher if sugar is taken between meals.
- On withdrawal of foods rich in sugar enhanced caries activity decreases.
- Caries can occur despite the avoidance of refined sugar and maximum restriction of natural sugar as well as dietary carbohydrates.
- An increase in the clearance time of sugar increases caries activity.
“Comparison of fluoride treatments vs non-fluoride alternatives”
Question 5. Write briefly on the caries vaccine.
Or
Write a short note on the caries vaccine.
Or
Write a short note on the dental caries vaccine.
Answer. The concept of vaccination against dental caries has existed almost the time as this disease was recognized to result from the colonization of teeth by acidogenic bacteria. Considerable progress has been made in elucidating the factors involved in their pathogenic activity, culminating recently in the sequence of the entire S. mutans genome.
Properties of an Ideal Dental Caries Vaccine
- Broad coverage for all common cariogenic S. mutans strains
- Should work for both high and low-risk populations.
- Could be given as a pan of another immunization (WHO effort is to reduce the number of vaccinations)
- Could be given by various routes and still be effective
- Inexpensive
- Delivered by individuals with little training
- It could provide “herd immunity”.
But because of different variations, more than one vaccine approach may ultimately be optimal to use.
Types of Caries Vaccines
Vaccines may be prepared from:
- Live modified organisms
- Inactivated or killed organisms
- Extracted cellular fractions, toxoid,s, oar r combination of these
Specific Vaccine Targets
There are several types of vaccine against dental caries in development, and these differ in terms of their target antigen. S. mutans posses various cell surface substances; adhesions, Glucosyltransferase, glucan binding proteins. These substances are useful for vaccine preparation.
Adhesin
Adhesins from the two principal human pathogens of S. mutans have been purified. Antigens I/2 are found in the culture supernatant as well as in the S. mutans cell surface. Abundant in vitro and in vivo evidence, using a variety of active and passive immunization approaches, indicates thatantibodiesy with specificity for mutans streptococcal adhesions can interfere with bacterial adherence and subsequent dental caries caused by S. mutans.
“Steps to improve oral hygiene for caries prevention”
Glucosyltransferase
S. mutans has three forms of glucosyltransferases (GTFs):
- Water-insoluble glucan-synthesizing enzyme; GTF-I
- Water-insoluble and water-soluble glucan synthesizing enzymes: GTF-S-I
- Water-soluble glucan synthesizing enzymes: GTF-S
The genes encoding GTF-I, GTF-S-I, and GTF-S are called the GTF-B, GTF-C, and GTF-D genes, respectively. All three GTF genes are important for smooth surface caries formation in the pathogen-free rat model system. Streptococcus sobrinus produces a water insoluble glucan—synthesizing enzyme GTF-S. Thus, the presence of antibody to GTF in the oral cavity prior to infection, can significantly influence the disease outcome, presumably by interference with one or more functional activities of the enzyme.
Glucan Binding Protein
S. mutans secretes at least three distinct proteins with glucan-binding activity: GBP-A, GBP-B, and GBP-C. Of the three S. mutans GBPs, only GBP-B has been shown to induce a protective immune response to experimental dental caries. GBP-A has a sequence of 563 amino acids. The molecular weight is 59.0 kDa. The carboxy-terminal 2/3 rd ofthe GBP-A sequence has significant homology with a putative glucan-binding region of S. mutans GTFs. The C-terminal region contains 16 repeating units, which represent the full glucan-binding domain of this protein. GBP-A has a greater affinity for water-soluble glucan than for water-insoluble glucan.
Dextranases
Dextran is an important constituent of early dental plaque. Dextranase is an enzyme produced by Streptococcus mutans. They destroy dextran and thus the bacteria can invade dextran rich early dental plaque. Dextranase, when used as an antigen can prevent the colonization of the organism in early dental plaque.
Risk of Using the Caries Vaccine
All vaccines, even if properly manufactured and administered, seem to have risks:
- The most serious is that sera of some patients with rheumatic fever show serological cross-reactivity between heart tissue antigens and certain antigens from hemolytic Streptococci.
- Antisera obtained from rabbits immunized with wholecells of S. mutans and with a high molecular weight protein antigen of S. mutans were reported to cross react with human heart tissues.
- Glucosyltransferase was also tested for cross-reactivity with human heart tissue, and the results were negative.
Further research showed that the C-terminal part of antigen I/2 contains an epitope, which is cross-reactive with human IgG, and although the clinical significance of this observation is unknown, it appears that this potentially harmful epitope should be excluded from a caries vaccine. The human IgG cross-reactive region is also present in other mutans streptococci,suchh as Streptococcus sobrinus, as well as in non-mutans streptococci.
“Role of brushing and flossing in reducing cavities”
Question 6. Write a short note on Dental caries.
Answer. Dental caries is an irreversible progressive microbial disease of the calcified tissues of the teeth, characterized by the demineralization of the inorganic portion and distortion of the organic substances of the tooth, which often leads to “cavitation”.
Question 7. Write a short note on nursing bottle caries.
Answer. According to Kroll, It is a syndrome characterized by severe caries pattern beginning with maxillary anterior teeth in a healthy bottle-fed infant or a toddler:
- It is a type of rampant caries, the cause of which is an unhealthy bottle-fed infant or toddler.
- It is seen in the 2 to 4-year age group.
- Early caries involvement of maxillary anterior teeth, maxillary and mandibular posterior teeth, and mandibular canines is seen.
- Mandibular incisors are unaffected due to protection by the tongue.
- It is seen as the white or dark brown collar of caries seen around the neck of incisors, which develops into faciolingual caries and may also fracture the tooth.
- History reveals, child put to bed at afternoon naps or night with a nursing bottle containing milk or sugar containing beverages. The child falls asleep and milk or sweetened liquid becomes pooled around maxillary anterior teeth. This provides an excellent culture medium for acidogenic microorganisms salivary flow is reduced during sleep and clearance of the liquid from the oral cavity is slowed.
- Management includes parent counseling, provisional restorations, diet assessment, caries activity test, constant re-evaluation, fluoride therapy, and recall once in 2 to 3 months.
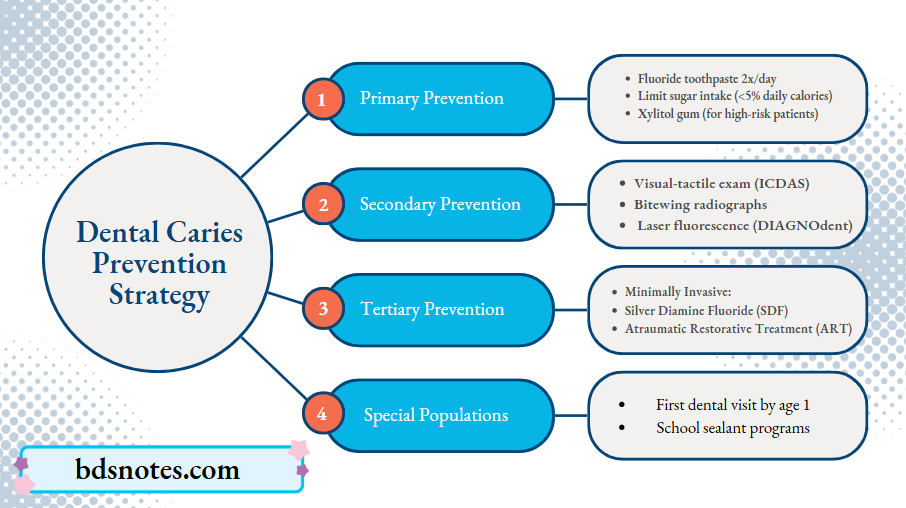
Question 8. Define primary prevention, secondary prevention. Write in detail about the prevention of dental caries.
Answer.
Definition of Primary Prevention
It is defined as “action taken before the onset of disease, which removes the possibility that a disease will ever occur”.
Definition of Secondary Prevention
It is defined as “an action that halts the progress of a disease at its incipient stage and prevents complications”.
Prevention of Dental Caries
“Early warning signs of poor oral hygiene leading to caries”
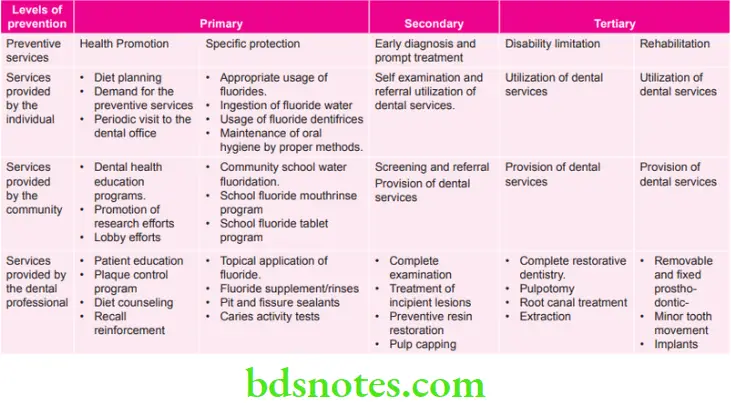
Question 9. Define prevention. Elaborate on the levels of prevention of dental caries and the iceberg phenomenon.
Answer.
Definition of Prevention
Prevention: It is defined as the efforts made to maintain normal developmental, physiological function and to prevent disease of the mouth and adjacent parts.
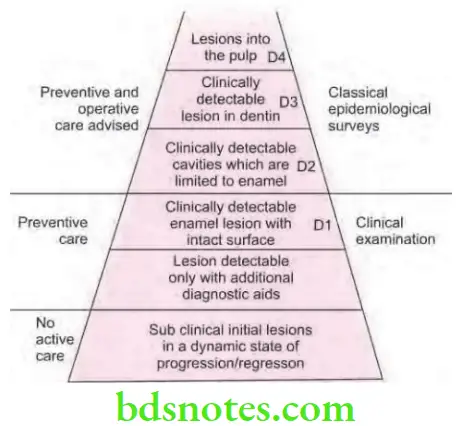
Iceberg Phenomenon
- As per the concept, disease in the community is compared with an iceberg.
- The floating tip of the iceberg represents what the doctor sees in the community, i.e., clinical cases.
- Vast submerged portion of iceberg represents the hidden mass of disease, i.e. latent, inapparent, presymptomatic and undiagnosed cases and carriers in the community.
- Waterline represents the demarcation between apparent and inapparent disease. Fig. 6: Iceberg for dental caries
- In various diseases like diabetes and hypertension, the submerged portion of an iceberg far exceeds the known morbidity.
- Hidden part of iceberg thus constitutes an important, undiagnosed reservoir of disease in community, its detection and control is a challenge to modern techniques in preventive medicine.
- Major deterrents in study of chronic diseases of unknown etiology is absence of methods to detect subclinical state, i.e. bottom of an iceberg.
“Asymptomatic vs symptomatic stages of caries development”
Question 10. Define primordial prevention. Enumerate the levels of prevention for dental caries.
Answer.
Definition of Primordial Prevention
Primordial prevention is the prevention of the emergence or development of risk factors in countries or population groups in which they have not yet appeared. The maintenance is by individual and mass education.
In primordial prevention, efforts are directed towards discouraging children from adopting harmful lifestyles.
“Treatment options for early-stage dental caries prevention”
Question 11. What is an epidemiological Write about the conclusions of classic diet and dental caries studies.
Answer.
Conclusion of Classic Diet and Dental Caries Studies
“Role of remineralization agents in preventing cavities”
Question 12. Enumerate studies conducted on diet and dental caries. Describe in detail the Vipeholm study.
Answer. Enumeration of studies conducted on diet and dental caries
- Vipeholm study
- Hopewood House study
- Turku sugar study
- Hereditary fructose intolerance
- Tristan Da Cunha study
“Follow-up care after implementing caries prevention strategies”
Question 13. Define epidemiology. Write in detail about the epidemiology of dental caries.
Answer. Epidemiology is “the study of the distribution and determinants of health-related states or events in specified populations and the application of this study to control health problems”.
Epidemiology of Dental Caries
- Studies have shown that dental caries remained low until the 17th century.
- Skeletal data shows that skulls of men from Pre-Neolithic period (12000 BC) did not exhibit dental caries but skulls from Neo-lithic period (12000-3000 BC) contained carious teeth.
- The prevalence of dental caries increased dramatically towards the end of 17th century and continued to increase until the early 1970. The only break in this increase came during the mid 40 and early 50s and this coincided with the reduced availability of sucrose as a result of food rationing imposed during the World War 2.
- Dental caries is a universal disease affecting all geographic regions, races, both the sexes and all age groups. The prevalence of dental caries is generally estimated at the ages of 5, 12, 15, 35 to 44 and 65 to 74 years for global monitoring of trends and international comparisons.
- The prevalence is expressed in terms of point prevalence (percentage of population affected at any given point in time) as well as DMFT index (number of decayed, missing and filled teeth in an individual and in a population).
- Since the mid 1970s reports from developed countries worldwide have shown that the prevalence of dental caries in children and adolescent has declined.
- WHO global data bank confirms a decline in the prevalence of dental caries in children and adolescents in developed countries, and there is an increase in dental caries in some developing countries.
- There is now increasing evidence that the incidence of caries levels has declined in developed countries in the past 20 years. Dental caries is now largely a disease affecting the deprived section of society.
- Recent reports also confirm that in many communities, 80% of dental caries is occurring in 20% of the population.
- The incidence of dental caries has been studied in American white populations. The results show dental caries to be the most prevalent chronic disease in this population. The disease affects all regardless of location, sex, age, or social stratum. The disease starts in young people just as soon as teeth erupt. About 90% of youngsters are affected by age 14. As mentioned earlier, however, the incidence of caries is decreasing in this young population in the U.S. and other Western countries. This downward trend is explained by increased fluoridation of community water supplies and by increased attention to regular care at dental offices and home.
- As per WHO global DMFT of 1.61 for 12 year olds in 2004, a reduction of 0.13 as compared to DMFT of 1.74 in year 2001. Percentage of countries having 3 DMFT or less is 74%, i.e. 139 countries.
- WHO reported a DMFT score of 3.94 for India in 2003. In India, there is evidence of increasing caries rate in children and adults. Dental caries has been consistently increasing both in prevalence and severity since last 5 decades.
- In India data from national oral health survey (2002–03) states that in children aged 12 years caries prevalence was 53.8% and mean DMFT was 1.8 whereas it was 80.2% and 5.4 in the 35–44 year age group. In 65–74 year age group, the prevalence was 85% and mean DMFT was 14.9.
Leave a Reply