Dural Folds Intracranial Dural Venous Sinuses And Pituitary Gland
Enumerate the dural folds (folds of dura mater).
Answer.
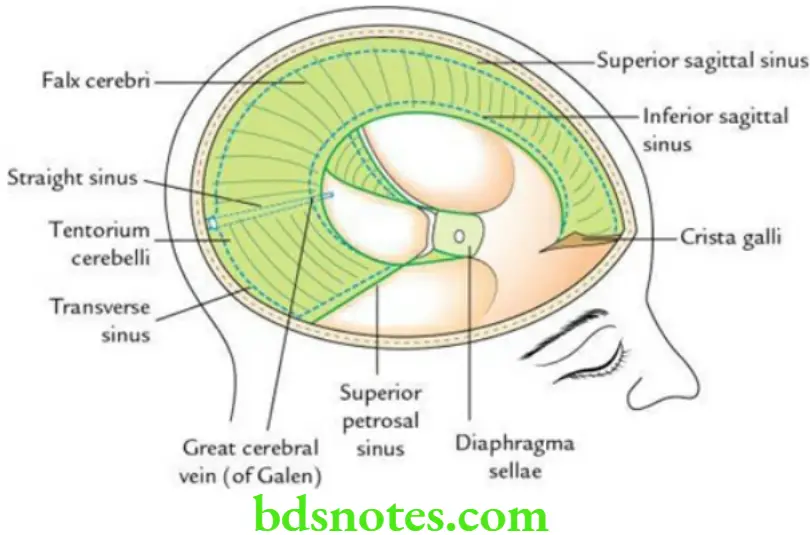
The dural folds are generally formed by folding of the meningeal layer of the cranial dura, which projects into the cranial cavity to divide it into various compartments, which lodge the different lobes/parts of the brain.
“Understanding the anatomy and function of the pituitary gland through FAQs: Q&A explained”
“Importance of studying dural folds and venous sinuses for medical students: Questions explained”
The folds of dura mater are as follows:
- Falx cerebri
- Tentorium cerebelli
- Falx cerebelli
- Diaphragma seller
Leave a Reply