Diseases Of The Pulp And Periapical Tissues Important Question And Answers
Question. Describe the etiology, histopathology, and clinical features of acute pulpitis.
Or
Describe etiology, histopathology, clinical features, and sequelae of acute pulpitis.
“Early warning signs of issues addressed by understanding pulp and periapical pathogenesis: Common questions”
Answer. Acute pulpitis is an irreversible condition characterized by an acute, intense inflammatory reaction in pulp tissue.
Etiology
- Pulp exposure due to faulty cavity preparation.
- Caries progressing beyond the dentinal barriers and reaching the pulp.
- Chemical irritation to pulp
- Cracked tooth syndrome
- Metallic restoration in a tooth without proper thermal insulation.
- A blow to the tooth with subsequent damage to the pulp.
- Recurrent caries around the preexisting restoration.
- Galvanic current produced due to dissimilar metallic restoration may be transmitted to pulp and cause pulpitis.
“Understanding the role of pulp and periapical diseases in oral health: Q&A explained”
Read And Learn More: Oral Pathology Question And Answers
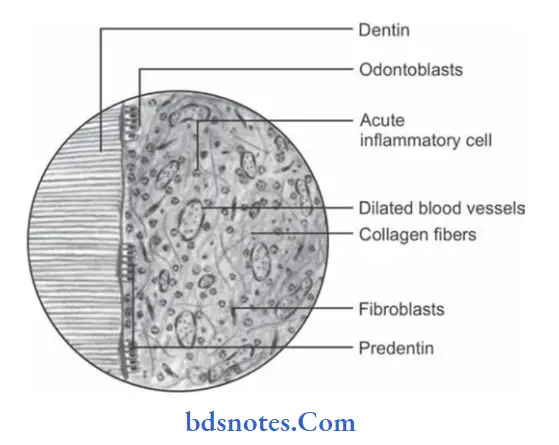
Histopathology
- Severe edema in the pulp with vasodilatation.
- Moderate to dense infiltration of polymorphonuclear leukocytes.
- Focal of destruction of odontoblast cells at pulp pulp-dentin border.
- Many micro abscess formations in pulp characterized by the area of liquefaction degeneration in pulp being surrounded by dense band of neutrophils and microorganisms.
“Importance of studying pulp and periapical diseases for better diagnostic outcomes: Questions explained”
“Common challenges in diagnosing pulp and periapical diseases effectively: FAQs provided”
- There may be complete liquefaction and necrosis of pulp with total destruction of the odontoblastic cell layer. This is known as acute suppurative pulpitis.
- The death of pulp is due to tissue dehydration. This is known as “dry gangrene of pulp”.
“Steps to explain causes of pulp diseases: Trauma vs caries: Q&A guide”
Clinical Features
- The tooth is sensitive to cold and hot stimuli.
- Application of hot or cold stimuli causes an increase in intensity to pain and such pain persists for longer duration even after the stimuli is removed.
- Intensity of pain increases during the sleep and occurs due to increase in local blood pressure in head and neck region.
- As the entrance of pulp is not wide, acute pulpitis helps in the spread of inflammation throughout pulp with subsequent necrosis.
- Acute pulpitis is often associated with microabscess formation in the pulp along with liquefaction degeneration.
Pain subsides when drainage is established or when pulp undergoes complete necrosis. - The tooth is nontender to percussion unless the pulpal inflammation has spread beyond the root apex into the periapical region.
- When intrapulpal pressure becomes very high during acute inflammation it cause collapse of apical blood vessels. This is known as “pulp strangulation”.
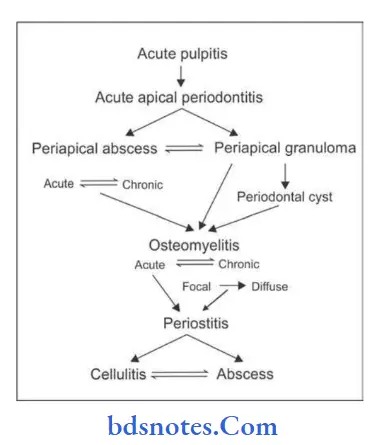
Sequelae Of Acute Pulpitis
“Role of bacterial infection in causing pulpitis: Questions answered”
Leave a Reply