Differences Between Primary And Secondary Healing
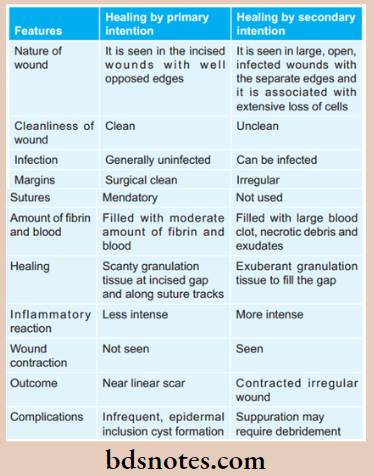
Question 1. Write the difference between the healing of wounds by primary and secondary intention.
Or
Give differences between primary and secondary healing.
Answer:
Question 2. Define inflammation and describe events in acute inflammation.
Answer:
Definition: Inflammation is defined as the local response of living mammalian tissues to injury due to any agent.
It is a body defense reaction in order to eliminate or limit the spread of injurious agent as well as to remove the consequent necrosed cells and tissues.
Difference between primary and secondary healing
Question 3. Write in detail the morphology, and pathogenicity of M. tuberculosis and write in detail about laboratory diagnosis of pulmonary tuberculosis.
Answer:
Pulmonary tuberculosis Morphology
- It is slender, gram-positive, acid-fast bacilli.
- It is non-sporing, non-capsulated, and non-motile.
- Slightly curved rod with granular or beaded staining.
- It occurs singly, in pairs, in bundles/clumps.
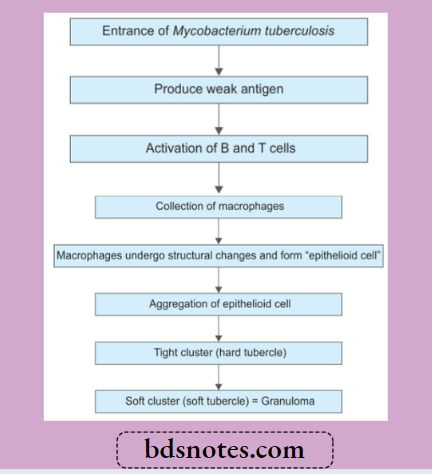
Pulmonary tuberculosis Pathogenicity
Pulmonary tuberculosis Diagnosis
1. Demonstration of AFB on microscopic examination of a diagnostic specimen (sputum or tissue): Smears or tissue slides stained by Ziehl-Neelsen stain are examined for acid fast bacilli. This method has a relatively low sensitivity in confirmed cases of pulmonary tuberculosis. Au-famine-rhodamine staining and fluorescence microscopy can improve the sensitivity to a certain extent. Three sputum specimens preferably collected early in the morning should be submitted to the laboratory for AFB smear and mycobacterial culture.
2. Culture: Besides sputum and tissue other specimens which can be used for culture are body cavity flids, urine or gastric lavage flid. Specimens may be inoculated onto egg or agar-based medium, e.g. Lowenstein-Jensen or Middlebrook 7H10 media and incubated at 37°C. M. tuberculosis grows slowly (4-8 weeks). A presumptive diagnosis can be made based on colony pigmentation and morphology; however, biochemical tests are must for species recognition.
3. Molecular typing: M. tuberculosis is isolated and species identification is done by molecular methods or high-pressure liquid chromatography of mycolic acids (reducing the time required for confirmation to 2-3 weeks). Polymerase chain reaction, i.e. PCR is the conformational method.
4. Tuberculin sensitivity test: It is based on the principle that M. tuberculosis in a concentrated liquid culture medium, i.e. purified protein extract can elicit a skin reaction when injected subcutaneously into patients with tuberculosis. A person is given the tuberculin and asked to return within 48-72 hours to have a trained healthcare worker to look for a reaction on the arm (swelling, induration and erythema) and measure its size. Redness by itself is not considered part of the reaction. The lack of mycobacterial species specificity, subjectivity of interpretation and batch-to-batch variations limit the usefulness of protein-purified derivatives.
Primary intention vs secondary intention healing
5. In vitro assays that measure T cell release of IFN-γ in response to stimulation with the highly tuberculosis-specific antigens ESAT6 and CPP10: These are commercially available assays (Interferon ? release assay or IGRA) IGRAs are more specific than the tuberculin sensitivity test as a result of less cross-reactivity due to BCG vaccination and sensitization by non-tuberculous mycobacteria. IG- RAs also appear to be at least as sensitive as the tuberculin-sensitive test for active tuberculosis.
6. Complete hemogram: It shows lymphocytosis and raised ESR.
7. Fine needle aspiration cytology: This is done in the enlarged peripheral lymph node and is easy way for confirmation of the diagnosis.
8. Immunohistochemistry: Immunohistochemical stain with anti-MBP 64 antibody stain can be used to demonstrate the organism.
Leave a Reply