Difference Between Thrombosis And Coagulation
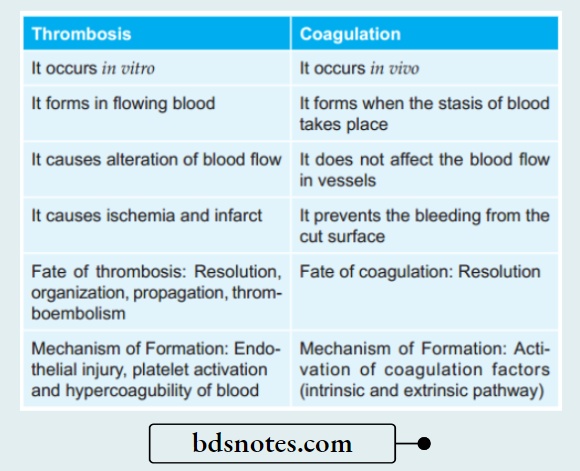
Question 1. How will you differentiate thrombosis and coagulation?
Answer:
Question 2. Write a short note on infarct.
Answer:
Infarction is the process of tissue necrosis resulting from some of circulatory insufficiency, the localized area of necrosis so developed is called as an infarct.
Infarct Etiology
- Most commonly infarcts are caused by interrupted arterial blood supply called ischemic necrosis.
- Less commonly venous obstruction can produce infarct termed as stagnant hypoxia.
- Generally, sudden complete and continuous occlusion by thrombosis or emboli produces infarcts.
- Infarcts may be produced by non-occlusive circulatory insufficiency.
Difference between thrombosis and coagulation
Types of Infarcts
Infarcts are classifid depending upon diffrent features:
- According to their color:
- Pale or anemic, due to arterial occlusion and are seen in compact organs, For Example. in the kidneys, heart, and spleen.
- Red or hemorrhagic, seen in soft loose tissues and are caused either by pulmonary arterial obstruction (For Example. in the lungs) or by arterial or venous occlusion ( For Example. in the intestines).
- According to their age:
- Recent or fresh
- Old or healed
- According to the presence or absence of infection:
- Bland, when free of bacterial contamination
- Septic, when infected.
Infarct Pathogenesis
The process of infarction takes place as follows:
- Localized hyperemia due to local anoxemia occurs immediately after obstruction of the blood supply.
- Within a few hours, the affected part becomes swollen due to edema and hemorrhage. The amount of hemorrhage is variable, being more marked in the lungs and spleen, and less extensive in the kidneys and heart.
- Cellular changes such as cloudy swelling and degeneration appear early (reversible cell injury), while cell death (irreversible cell injury or necrosis) occurs in 12-48 hours.
- There is progressive proteolysis of the necrotic tissue and there is lysis of the red cells.
- An acute inflammatory reaction and hyperemia appear at the same time in the surrounding tissues in response to products of proteolysis.
- Blood pigments, hematoid and hemosiderin, liberated by the lysis of RBCs are deposited in the infarct. At this stage, most infarcts become pale grey due to the loss of red cells.
- Following this, there is a progressive in the growth of granulation tissue from the margin of the infarct so that eventually the infarct is replaced by a fibrous scar. Dystrophic calcification may occur sometimes.
Thrombosis definition in pathology
Morphologic Features
Some general morphological features of infarcts are:
Gross Features
- Infarcts of solid organs are usually wedge-shaped, the apex pointing towards the occluded artery and the wide base on the surface of the organ.
- Infarcts due to arterial occlusion are generally pale while those due to venous obstruction are hemorrhagic.
- Most infarcts become pale later as the red cells are lysed but pulmonary infarcts never become pale due to the extensive amount of blood.
- Cerebral infarcts are poorly defined with central softening (encephalomalacia).
- Recent infarcts are generally slightly elevated over the surface while the old infarcts are shrunken and depressed under the surface of the organ.
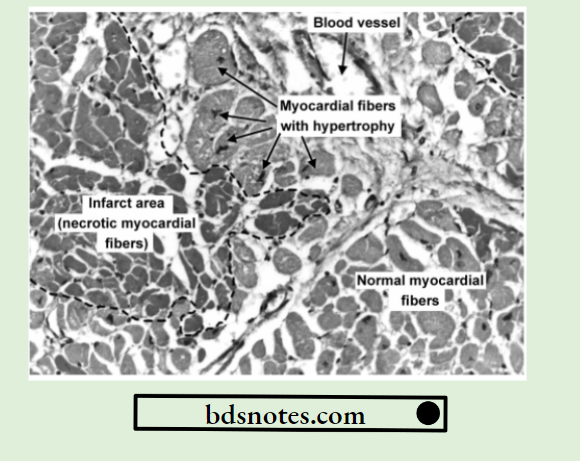
Microscopic Features
- Pathognomonic cytologic change in all infarcts is coagulative (ischemic) necrosis of the affected area of tissue or organ. In cerebral infarcts, however, there is characteristic liquefactive necrosis.
- Some amount of hemorrhage is generally present in any infarct.
- At the periphery of an infarct, an inflammatory reaction is noted. Initially, neutrophils predominate but subsequently, macrophages and fibroblasts appear.
- Eventually, the necrotic area is replaced by fibrous scar tissue, which at times may show dystrophic calcification.
- In cerebral infarcts, the liquefactive necrosis is followed by gliosis, i.e. replacement by microglial cells distended by fatt material (gitter cells).
Leave a Reply