Dental Implants
Write short note on osseointegration.
Or
Describe osseointegration.
Or
Write short answer on osseointegration.
Answer.
Osseointegration Introduction or Osseointegration Definition
Osseointegration Of Dental Implants
“Common challenges in achieving successful osseointegration”
- In the 1950s, Per-Ingvar Brånemark, a Swedish professor of anatomy, had a serendipitous finding while studying blood circulation in bone that became a historical breakthrough in medicine. He discovered an intimate bone-to-implant apposition with titanium that offered sufficient strength to cope with load transfer. He called the phenomenon osseointegration and developed an implant system with a specific protocol to predictably achieve it.
- Histologically, osseointegration is defined as the direct structural and functional connection between ordered, living bone and the surface of a load-bearing implant without intervening soft tissues.
- Clinically, osseointegration is the rigid fixation of an alloplastic material (implant) in bone with the ability to withstand occlusal forces.
“Understanding the role of osseointegration in implant success”
- Branemark also stated that the implant should not be loaded during healing period for osseous integration to occur.
- Osseointegration is a clinically asymptomatic rigid fixation of the implant within bone, during functional loading.
- There is no connective tissue intervening between bone and implant so the interface is strong one which can withstand the occlusal loads.
- Interface consists of remodeled bony tissue. To develop this strong interface, the implant should not be overloaded during its organization period (Soon after placement of implant).
- During this period, the surgical area undergoes a remodeling process just like an extraction site.
- During organization the bone grows into the irregularities of the implant surface
- Hydroxyapatite coated implant get “Biointegrated” with the bone tissue.
“Importance of studying osseointegration for dental professionals”

“Steps to explain the biological process of osseointegration”
Read And Learn More: Periodontics Question And Answers
Basic Principles of Implant Therapy to Achieve Osseointegration
- Implants must be sterile and made of a biocompatible material (e.g., titanium).
- Implant site should be prepared under sterile conditions.
- Implant site should be prepared with an atraumatic surgical technique that avoids overheating of the bone during preparation of the recipient site.
- Implants should be placed with good initial stability.
- Implants should be allowed to heal without loading or micromovement (i.e., undisturbed healing period to allow for osseointegration) for 2 to 4 or 4 to 6 months, depending on the bone density, bone maturation, and implant stability.
“Role of bone cells like osteoblasts and osteoclasts in osseointegration”
Stages of Osseointegration or Osseointegration Process
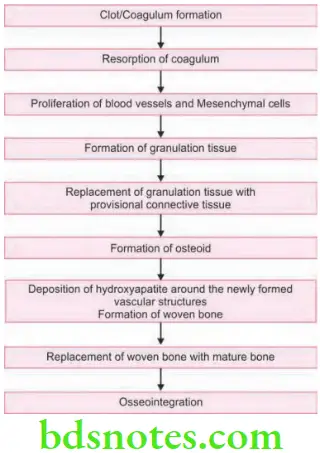
“Early warning signs of failed osseointegration”
Factor Affecting Osseointegration
Overload: It causes failure of osseointegration. Premature loading of implant at the time of healing leads to fibrous encapsulation and not osseointegration.
“Steps to teach students about osseointegration of dental implants”
- Biocompatibility of the material.
- Implant design: Most conductive design for osseointegration is cylindrical.
- Implant surface: Implant with mild surface roughness leads to more osseointegration.
- Surgical site: A healthy site is required previously irradiated area is contraindicated.
“Asymptomatic vs symptomatic stages of osseointegration issues”
- Surgical technique: Minimum possible trauma. Surgical drilling should be intermittent, slow rate and is by using sharp instrument.
- Infection control: Infection especially form the periodontium should be avoided.
Leave a Reply