Corticosteroids Question And Answers
Question 1. Discuss Glucocorticoids.
Answer:
Glucocorticoid is a corticosteroid and it is secreted from the adrenal cortex.
“Understanding the role of corticosteroids in treating inflammation”

“Importance of studying corticosteroids for healthcare professionals”
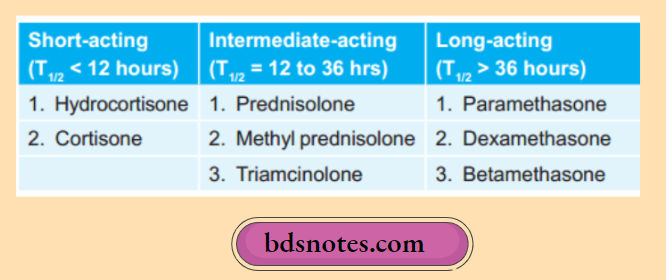
Classification Of Glucocorticoids
Read And Learn More: Pharmacology Question And Answers
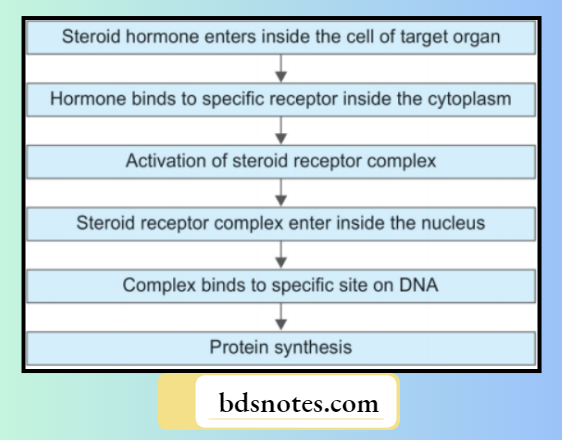
Glucocorticoids Mechanism Of Action
“Common challenges in managing conditions with corticosteroids”
Action Of Glucocorticoids
- Carbohydrate metabolism: It promotes glycogenesis, and gluconeogenesis and decreases glucose utilization by peripheral tissues.
- Lipid metabolism: Chronic use of glucocorticoids leads to the redistribution of body fats.
- Protein metabolism: Glucorticoids lead to the breakdown of protein and mobilization of amino acids from muscle, skin, bone, etc. This leads to osteoporosis, thinning of the skin, growth retardation, etc. Wound healing and fibrosis are also inhibited.
- Electrolyte and water metabolism: Glucocorticoids have weak mineralocorticoid action which leads to retention of both sodium and water and increases excretion of potassium. So chronic use of these drugs leads to edema and hypertension.
- Calcium metabolism: Glucocorticoids cause inhibition of calcium absorption from the gut and increase renal excretion of calcium which causes a decrease in blood calcium level. This causes osteoporosis and pathological fracture of vertebral bodies.
“Signs of reduced inflammation with corticosteroids”
- Cardiovascular system: Glucocorticoids lead to the retention of sodium and water and create pressure acting on adrenaline and angiotensin. Long-term use of drugs can cause hypertension and worsening of congestive heart failure.
- Skeletal muscle: Glucocorticoids are required for normal muscle activity. Long-term use of glucocorticoids can cause muscle wasting as well as weakness.
- Central nervous system: Glucocorticoid therapy may lead to euphoria, insomnia, restlessness, and psychosis.
- Gastrointestinal tract: Glucocorticoid inhibits the secretion of prostaglandins which causes an increase in gastric acid and aggravates a peptic ulcer. Glucocorticoids also decrease the local immune response against H. pylori which increases the chances of peptic ulcer.
- Anti-inflammatory effect: They suppress inflammatory response thus they decrease capillary permeability, exudation, central infiltration, and phagocytic activity, and thus the sign of inflammation are reduced.
- Immunosuppressant effect: Glucocorticoids provide an immunosuppressant effect that causes inhibition of both B cell and T cell lymphocyte functions which leads to impairment of humoral and cell-mediated immunity.
Corticosteroids Tablets
The following are the therapeutic uses of glucocorticoids:
1. Endocrinal uses.
- Replacement therapy
- Acute adrenal insufficiency: Since it is a medical emergency that occurs due to infection or due to sudden withdrawal of steroids, it is treated with IV hydrocortisone hemisuccinate 100 mg bolus.
- Chronic adrenal insufficiency or Addison’s disease: This condition is treated by oral hydrocortisone 20 to 40 mg daily along with adequate salt and water.
“Role of glucocorticoid receptors in corticosteroid action”
2. Non-endocrinal uses.
- Rheumatoid arthritis: It provides immediate relief in rheumatoid arthritis but does not stop the progress of the disease. The steroid is given along with NSAIDs. If one or two joints are involved intra-articular injection is given.
- Osteoarthritis: In the acute form of the disease intra-articular injection is given.
- Rheumatic fever: Glucocorticoids provide more symptomatic relief and are indicated in cases with carditis and congestive cardiac failure.
- Gout: Glucocorticoids are used in cases with acute gout when NSAIDs don’t work.
- Allergic conditions: Glucocorticoids suppress allergic conditions such as hay fever, drug reactions, urticaria, contact dermatitis, angioneurotic edema, and anaphylaxis. Glucocorticoids are slow-acting drugs in these allergic conditions.
- Bronchial asthma: In acute status asthmaticus, IV hydrocortisone is given. In chronic asthma, inhalational preparations such as beclomethasone, and budesonide should be given.
“Treatment options for conditions requiring corticosteroids”
- Collagen diseases: In collagen diseases such as polyarteritis nodosa, dermatomyositis, etc. large doses of glucocorticoids provide good relief.
- Renal disease: Glucocorticoids act as first-line drugs in nephrotic syndrome.
- Eye diseases: Corticosteroids are used in many inflammatory ocular diseases and prevent damage to vision.
- Dermatological diseases: Topical glucocorticoids provide relief from the itching, pain, and inflammation of various dermatological diseases. Systemic steroidal therapy acts as life-saving in Steven Johnson syndrome, Pemphigus vulgaris, etc.
- Hematological diseases: Glucocorticoids have good control over autoimmune hemolytic anemias. Since glucocorticoids provide lymphocytic action they are indicated in various malignancies, leukemias, and Hodgkin’s disease.
- Cerebral edema: Dexamethasone has the mechanism of not retaining salt and water, so it is the first choice of steroid in cerebral edema.
- Gastrointestinal diseases: Methylprednisolone is used in severe cases.
- Lung diseases: Glucocorticoids are useful in the treatment of aspiration pneumonia and infant respiratory distress syndrome.
- Shock: In septic shock IV glucocorticosteroids are given as life-saving drugs.
- Organ transplantation: Glucocorticoids are useful to treat and prevent graft rejection. Other uses of corticosteroids are in Bell’s palsy, myotonia, and acute polyneuritis.
“Role of combination therapies in managing refractory symptoms”
Question 12. Write A Basis Of Use Of Glucocorticoids In Inflammatory Condition.
Answer:
Glucocorticoids provide anti-inflammatory effects in inflammatory conditions.
- Glucocorticoids induce a protein known as lipocortin which causes inhibition of enzyme phospholipase A2 due to which prostaglandins, leukotrienes, and platelet-activating factors are not formed which leads to inflammation.
- Cytokines such as interleukin 1 and 6 as well as TNF-α get inhibited which leads to inflammation.
- Glucocorticoids also stabilize the lysosomal membrane and prevent the release of inflammatory mediators.
- Glucocorticoids stop the production of adhesion molecules from both endothelial cells and macrophages and decrease the migration of neutrophils at the site of injury.
- In conclusion, they suppress early phenomena i.e. capillary permeability, edema, cellular infiltration, and phagocytosis which prevent inflammation.
Corticosteroids Drugs
“Follow-up care after initiating corticosteroid therapy”
Question 14. Enumerate Inhalational Glucocorticoids. Write Down The Therapeutic Uses And Adverse Effects Of Corticosteroids.
Answer:
Enumeration of inhalational glucocorticoids
- Beclomethasone dipropionate
- Budesonide
- Fluticasone propionate
- Flunisolide
- Ciclesonide.
“Complications of ignoring chronic inflammation”
Therapeutic uses Of Corticosteroids
1. Endocrinal uses.
- Replacement therapy
- Acute adrenal insufficiency: Since it is a medical emergency that occurs due to infection or due to sudden withdrawal of steroids, it is treated with IV hydrocortisone hemisuccinate 100 mg bolus.
- Chronic adrenal insufficiency or Addison’s disease: This condition is treated by oral hydrocortisone 20 to 40 mg daily along with adequate salt and water.
2. Non-endocrinal uses.
- Rheumatoid arthritis: It provides immediate relief in rheumatoid arthritis but does not stop the progress of the disease. The steroid is given along with NSAIDs. If one or two joints are involved intra-articular injection is given.
- Osteoarthritis: In the acute form of the disease intra-articular injection is given.
- Rheumatic fever: Glucocorticoids provide more symptomatic relief and are indicated in cases with carditis and congestive cardiac failure.
- Gout: Glucocorticoids are used in cases with acute gout when NSAIDs don’t work.
- Allergic conditions: Glucocorticoids suppress allergic conditions such as hay fever, drug reactions, urticaria, contact dermatitis, angioneurotic edema, and anaphylaxis. Glucocorticoids are slow-acting drugs in these allergic conditions.
- Bronchial asthma: In acute status asthmaticus, IV hydrocortisone is given. In chronic asthma, inhalational preparations such as beclomethasone, and budesonide should be given.
- Collagen diseases: In collagen diseases such as polyarteritis nodosa, dermatomyositis, etc. large doses of glucocorticoids provide good relief.
- Renal disease: Glucocorticoids act as first-line drugs in nephrotic syndrome.
“Pathophysiology of untreated inflammation explained”
- Eye diseases: Corticosteroids are used in many inflammatory ocular diseases and prevent damage to vision.
- Dermatological diseases: Topical glucocorticoids provide relief from the itching, pain, and inflammation of various dermatological diseases. Systemic steroidal therapy acts as life-saving in Steven Johnson syndrome, Pemphigus vulgaris, etc.
- Hematological diseases: Glucocorticoids have good control over autoimmune hemolytic anemias. Since glucocorticoids provide lymphocytic action they are indicated in various malignancies, leukemias, and Hodgkin’s disease.
- Cerebral edema: Dexamethasone has the mechanism of not retaining salt and water, so it is the first choice of steroid in cerebral edema.
- Gastrointestinal diseases: Methylprednisolone is used in severe cases.
- Lung diseases: Glucocorticoids are useful in the treatment of aspiration pneumonia and infant respiratory distress syndrome.
- Shock: In septic shock IV glucocorticosteroids are given as life-saving drugs.
- Organ transplantation: Glucocorticoids are useful to treat and prevent graft rejection. Other uses of corticosteroids are in Bell’s palsy, myotonia, and acute polyneuritis.
Adverse effects Of Corticosteroids
- Cushing’s habitus: Abnormal fat distribution which leads to characteristic appearance with a rounded face, narrow mouth, supraclavicular hump, obesity of trunk with relatively thin limbs.
- The fragile skin and purple striae: Present typically on thighs and lower abdomen, easy bruising, telangiectasis, hirsutism. Cutaneous atrophy localized to the site occurs with topical application as well.
- Hyperglycemia: It may be glycosuria or the precipitation of diabetes.
- Muscular weakness: Proximal (shoulder, arm, pelvis, thigh) muscles are primarily affected. Myopathy occurs occasionally, and warrants withdrawal of the corticoids.
- Susceptibility to infection: Long-term therapy with steroids leads to the fire-up of opportunistic infections like viral, fungal, and bacterial.
- Delayed healing: There is delayed healing of wounds and surgical incisions.
- Peptic ulceration: Risk is doubled; bleeding and silent perforation of ulcers may occur. Dyspeptic symptoms are frequent with high-dose therapy.
“Emerging research on advanced corticosteroid treatments”
- Osteoporosis: Especially involving vertebrae and other flat spongy bones. Compression fractures of vertebrae and spontaneous fractures of long bones can occur, especially in the elderly.
- Avascular necrosis: Avascular necrosis of the head of the femur, humerus, or knee joint is an occasional abrupt onset complication of high-dose corticosteroid therapy.
- Eye: Posterior subcapsular cataracts may develop after several years of use, especially in children. Glaucoma may develop in susceptible individuals after prolonged topical therapy.
- Growth retardation: It occurs in children even with small doses if given for long periods. Large doses do inhibit growth hormone secretion, but growth retardation may, in addition, be a direct cellular effect of corticoids. Recombinant growth hormone given concurrently can prevent growth retardation, but the risk/benefit of such use is not known.
- Psychiatric disturbances: The presence of mild euphoria frequently accompanies high-dose steroid treatment. This may rarely progress to manic psychosis. Nervousness, decreased sleep, and mood changes occur in some patients. Rarely a depressive illness may be induced after long-term use.
- Suppression of hypothalamo—pituitary—adrenal (HPA) axis: This occurs depending both on the dose and duration of therapy. In time, adrenal cortex atrophies and stoppage of exogenous steroids precipitates withdrawal syndrome consisting of malaise, fever, anorexia, nausea, postural hypotension, electrolyte imbalance, weakness, pain in muscles and joints, and reactivation of the disease for which they were used. Subjected to stress, these patients may go into acute adrenal insufficiency leading to cardiovascular collapse.
“Global prevalence of inflammatory diseases and their management”
Question 15. Explain Why Sudden Withdrawal Of Glucocorticoids After Prolonged Therapy Is Contraindicated.
Answer:
Glucocorticoids should not suddenly undergo withdrawal after prolonged therapy because:
- It can cause a flare of underlying clinical conditions for which they are being administered.
- Steroids after long-term use can result in hypothalamopitutary adrenal axis suppression but because exogenous steroids are being administered, no symptoms occur. Abrupt discontinuation of steroids can result in acute adrenal insufficiency.
- Sudden withdrawal of glucocorticoids is associated with the development of nonspecific features like fever, myalgia, and malaise. This can mimic the features of connective tissue disorders.
- Withdrawal of glucocorticoids is rarely associated with pseudotumor cerebri i.e. a condition characterized by increased intracranial pressure with papilledema.
“Case studies on outcomes of corticosteroid therapies”
Question 16. Why Are Glucocorticoids Avoided In Patients With Active Peptic Ulcer Disease?
Answer:
Glucocorticoids are avoided in patients with active peptic ulcer disease because glucocorticoids inhibit prostaglandins which leads to an increase in gastric acid and pepsin secretion which aggravate the peptic ulcer. They also lead to bleeding and silent perforation of peptic ulcer.
Leave a Reply