Burn Important Question And Answers
Important Question And Answers
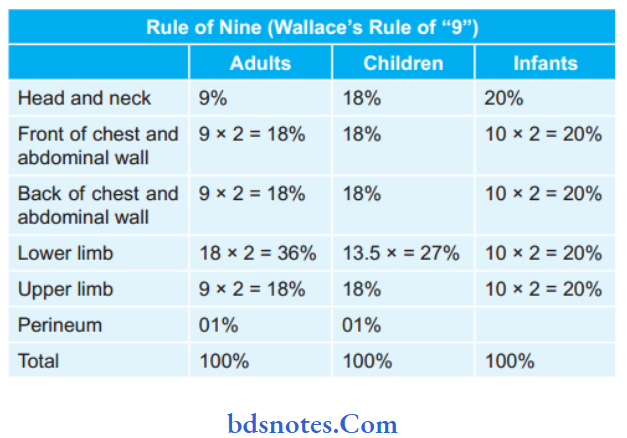
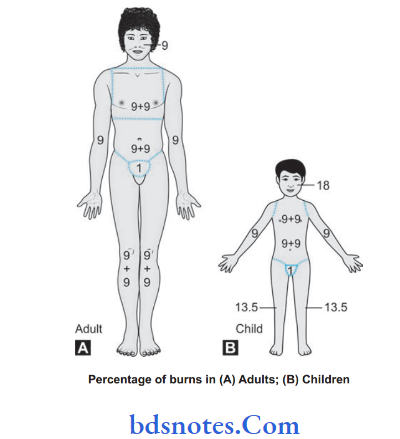
Question 1. What is Wallace’s rule of nine? Calculate the amount of fluid that should be ideally transfused to an adult weighing 60 kg and having 50% deep burns in the first 24 hours.
Answer. Wallace’s rule of nine is given by Wallace for early assessment of the extent of the burn in terms of body surface area.
“How To Care For A Burn Blister”

“What Are The Stages Of Burn Healing“
Burn: A burn is a wound in which there is coagulative necrosis of tissue.
“Can Burns Cause Nerve Damage”
Read And Learn More: General Surgery Questions and Answers
The amount of fluid that should be ideally transfused in case of burn is calculated by:
“Effective Home Remedies For Minor Burns”
Burn Muir and Barclay Formula
1 ration =% of burn × Body weight (kg)/2
3 rations in 12 hours, 2 rations in the next 12 hours, and 1 ration in the next 12 hours.
50% burns patients weighing 60 kg
“Comprehensive Overview Of Burn Degrees“
1 ration = 50 × 60/2= 1500 mL
1st 12 hours: 1500 × 3 = 4500 mL
2nd 12 hours: 1500 × 2 = 3000 mL
Total 7500 mL fluid in 24 hours.
Leave a Reply