Brachial Plexus
Question 1. Describe the brachial plexus under the following headings: (a) formation, (b) components, (c) location, (d) branches, and (e) applied anatomy.
Answer.
Brachial Plexus Formation
“Understanding the brachial plexus through FAQs: Composition, functions, and uses explained”
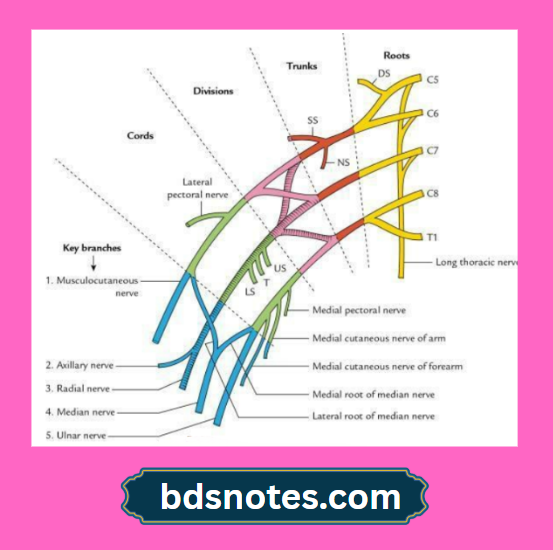
Brachial Plexus is formed by the ventral primary rami of C5, C6, C7, C8, and T1.
“Importance of studying the brachial plexus for medical students: Questions explained”
Brachial Plexus Components
The brachial plexus consists of four components:
- Roots
- Trunks
- Divisions
- Cords
Brachial Plexus Location
- Roots and trunks lie in the root ofthe neck.
- Divisions lie behind the clavicle.
- Cords lie in the axilla.
Brachial Plexus Branches
From roots
- Dorsal scapular nerve (C5) for rhomboids.
- Nerve to the serratus anterior (C5, C6, and C7) for the serratus anterior, as the name implies.
From the trunk (only the upper trunk gives branches)
- Suprascapular nerve (C5 and C6) for supraspinatus and infraspinatus muscles.
- Nerve to the subclavius.
“Common challenges in mastering brachial plexus notes effectively: FAQs provided”
From cords
- Lateral cord
- Lateral pectoral nerve (C5–C7)
- Lateral root of median nerve (C5–C7)
- Musculocutaneous nerve (C5–C7)
Mnemonic: Laila Loved Majnu.
- Medial cord
- Medial pectoral nerve for pectoralis major and pectoralis minor
- Medial cutaneous nerve of the arm
- Medial cutaneous nerve of the forearm
- Medial root of median nerve
- Ulnar nerve
- Posterior cord
- Upper subscapular nerve for the subscapularis muscle
- The lower subscapular nerve for the subscapularis and teres major muscles
- Nerve to latissimus dorsi (thoracodorsal nerve)
- Axillary nerve for the deltoid and teres minor muscles
- Radial nerve
Mnemonic: ULNAR
Brachial Plexus Applied Anatomy
“Factors influencing success with brachial plexus studies: Q&A”
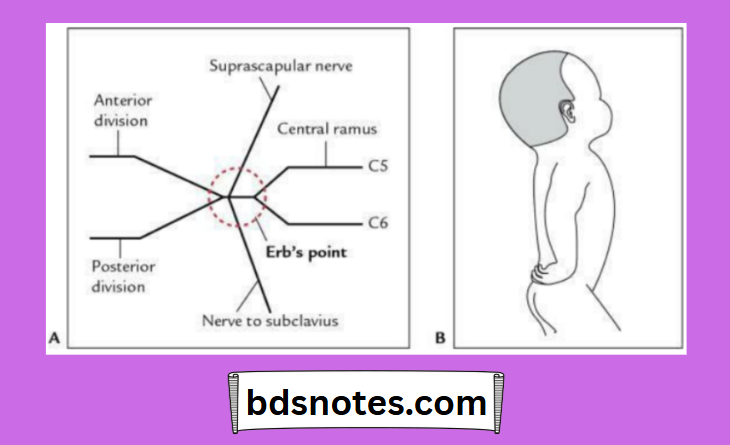
- Erb’s paralysis: It occurs due to injury of the upper trunk of the brachial plexus at Erb’s point.
- Klumpke paralysis: It occurs due to injury to the lower trunk of the brachial plexus.
- Horner syndrome: It occurs due to involvement of the sympathetic fibres.
- Winging of the scapula: It occurs due to injury of the nerve to the serratus anterior.
Erb paralysis
- Site of injury: Erb’s point (the region of the upper trunk where six nerves meet, i.e., ventral rami of C5 and C6, anterior and posterior divisions of the upper trunk, and suprascapular nerve and nerve to subclavius).
- Cause: Undue (i.e, too much) separation of head from shoulder, e.,g. (a) pulling of fetal head by forceps during delivery (birth injury) and (b) fall on the shoulder.
- Clinical features:
- Arm hangs by the side. It is adducted and medially rotated, i.e. person is unable to abduct and laterally rotate the arm.
- Forearm is extended and pronated, i.e. person is unable to flex and supinate the forearm.
- Loss of sensation over a small area on the lower part of the deltoid.
“Why is proper understanding of the brachial plexus critical for diagnosing nerve injuries? Answered”
Klumpke paralysis
- Site of injury: Lower trunk of brachial plexus involving C8 and T1, mainly T1.
- Causes: Undue abduction of arm from body, e.g., (a) birth injury (pulling of upper limb during delivery), (b) reflex catching of something with hand while falling from a height, i.e. branch of a tree while falling from a tree.
- Clinical features:
- Claw hand, due to paralysis of the intrinsic muscles of the hand
- Sensory loss along the medial border of of the forearm and hand
- Horner syndrome is due to involvement of the sympathetic nerve to the head and neck
Leave a Reply