Bacterial Infections Of Oral Cavity Important Question And Answers
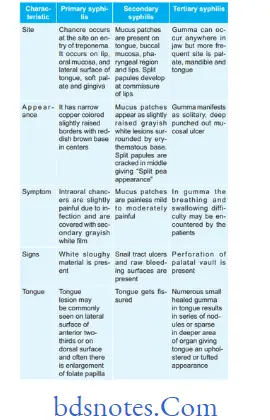
Question.1. Write notes on oral manifestations of syphilis.
Bacterial infections of oral cavity
Answer. Oral manifestations of syphilis are given below:
“Steps to explain the causes of bacterial infections in the oral cavity: Plaque vs poor hygiene: Q&A guide”
“Understanding the role of bacteria in oral health: Q&A explained”
Question.2. Describe oral manifestations of leprosy, tuberculosis and syphilis.
Answer.
Oral Manifestations Of Leprosy
- In oral cavity, the disease produces tumor-like lesions called “lepromas” which are found on lips, gingiva, tongue and hard palate.
- Oral lesion appears as yellowish soft or hard sessile growth which have tendency to break down and ulcerate.
- Ulceration, necrosis and perforation of palate.
- Fixation of palate with loss of uvula.
“Common challenges in diagnosing bacterial infections of the oral cavity effectively: FAQs provided”
- Difficulty in swallowing and regurgitation.
- Cobblestone appearance of tongue with loss of taste sensation.
- Chronic gingivitis, periodontitis and candidiasis are present.
- Enamel hypoplasia of teeth, pinkish discoloration of teeth and tapering of teeth is present.
Read And Learn More: Oral Pathology Question And Answers
“Importance of studying bacterial infections for better oral health outcomes: Questions explained”
Oral Manifestations Of Tuberculosis
- Tuberculous infection in oral cavity may produce nodules,vesicles, fisures, plaque, granulomas or verrucal papillary lesions.
- Tuberculous lesions of oral cavity are tuberculous ulcers,tuberculous gingivitis and tuberculosis of salivary gland.
- Tongue is most common location for the occurrence, besides this palate, gingiva, lips, buccal mucosa, alveolar ridge and vestibules may also be affcted.
- Tongue lesion: Tuberculous lesion of tongue develops on the lateral borders and appears as single or multiple ulcers which are well defied, painful, fim and yellowish gray in color.
- Lip lesions: Lesions produce small, nontender, granulating ulcer at mucocutaneous junction.
- Gingival lesions: These lesions produce small granulating ulcers with concomitant gingival hyperplasia.
- Tuberculous lesion of jaw bone: Chronic osteomyelitis of maxilla and mandible may occur and infection reaches to bone via blood or root canal or extraction socket.
Tuberculous osteomyelitis of jaw bone produces pain,swelling, sinus or fitula formation.
Leave a Reply