Antianginal And Other Anti-Ischemic Drugs Question And Answers
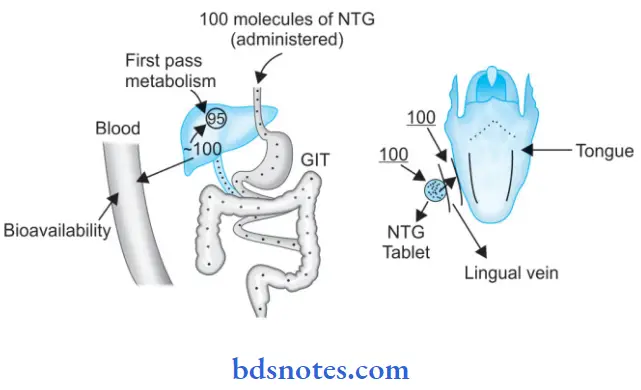
Question 1. Give The Pharmacological Explanation For Why Nitroglycerine Tablet May Not Be Effective When Swallowed, But Works Very Well For Patient Of Angina Pectoris When Kept Under The Tongue?
Or
Explain Why Nitroglycerin Is Used Sublingually In The Treatment Of an Acute Attack Of Angina Pectoris.
Answer:
Nitroglycerine has a very high first-pass metabolism. So the drug achieves a low plasma concentration when given orally. Thus, its bioavailability is less through the oral route. To circumvent this drug is administered by the sublingual route.
Through the sublingual route drug directly reaches the blood vessel and has a faster onset of action to stop an acute attack of angina.
Antianginal Drugs: Mechanism, Uses, and Side Effects
“Importance of studying antianginal drugs for healthcare professionals”
Read And Learn More: Pharmacology Question And Answers
Self-administration of drugs is possible by sublingual route.
“Understanding the role of antianginal drugs in treating ischemic heart disease”
Mechanism Of Action
Nitrates cause smooth muscle relaxation of veins and cause peripheral pooling of blood and reduce venous return, decrease preload, end-diastolic size, and pressure is decreased due to which cardiac work is reduced.
Anti-Ischemic Drugs: Treatment Options and Dosage
“Techniques for managing high-risk groups with ischemic heart disease”
Question 2. Explain why β-blockers are Not Used In Stable Angina Pectoris.
Answer:
β-blockers exacerbate stable angina due to unopposed α-mediated coronary constriction that may accentuate coronary spasm. That’s why they are not used in stable angina patients.
Leave a Reply