General Medicine Practicals
Name :
Age :
Sex :
Address :
Occupation :
Religion :
Socio-economic status :
Marital status :
Date of admission :
History:
Chief complaints:
Chief complaints History of present illness:
1. Past history
- Medical
- Surgical
2. Personal history
- Marital status: s/m/w no. of children
- Habit: tobacco/snuff alcohol
- Diet: mixed veg non-veg
- Lifestyle: sedentary non-sedentary
- Drug allergies
3. Family history
- Mother
- Father
- Siblings
- H/o DM BP
- Heart CVA
- Allergies
- Cancer
- Epilepsy
- Endocrine and others.
4. Drug history
5. History of immunisation.
Chief complaints Systemic review:
6. Cardio-vascular system
- Chest pain
- Breathing difficulty
- Palpitation
- Swelling feet
- History of hypertension, any medication
General Medicine Practicals Guide
7. Respiratory system
- Sneezing
- Cough
- Dyspnoea
- Wheezing
- Running nose
- Sputum
- Nose block
8. Gastro-intestinal system
- Appetite
- Abdominal pain
- Flatulence and dyspepsia
- Bowel habit
- Peptic ulcer
9. Genito-urinary system
- Frequency: Day night
- Burning: Start throughout ending
- Urgency: Hesitancy dribbling overnight
- Prostrate enlargement
- Hydrocele
- Hernia
10. Central nervous system
- Headache: Subjective objective aur
- Giddiness
- Memory and concentration
- Neuritis
- Sleep
11.Eyes
- Vision
12. Ear
- Hearing
- Pain
- Discharge
13.Skin
- Colour
- Dry/moist
- Scaly / smooth/ rough
14. General symptom
15. Present medication
- Physical Examination
Chief complaints General:
Chief complaints General CVS:
CVS Heart Rate:
- Rhythm
- Regularity
CVS Bp:
- Supine
- Sitting
- Standing
CVS Heart Sound:
- Murmur
- Thrill
Apex beat.
CVS RS:
1. Appearance of chest
- Shape
- Symmetry
2. Wasting of muscles
3. Drooping of shoulders.
- Rate and Type
- Breath Sound
- Apex beat
CVS Abdomen:
- Appearance-Spleen-Kidney
- Liver-Colon-Tenderness
- Bowel Sounds +/-
- Movements
CNS:
- Consciousness-Speech
- Cranial nerves-Sensory system
- Motor system-Reflexes
Genito-urinary system:
Provisional diagnosis:
Differential diagnosis:
Date:
Signature of medical officer
Cardiovascular System
Case Proforma:
Name : For identification
Age : Rheumatic fever commonly manifests < 15 year of age
: Degenerative and arteriosclerotic changes occur in old age
: Congenital diseases
: ASD at 6 months of age manifested
: VSD 6-10 weeks of age
: PDA 6 – 10 weeks of age.
Sex : In rheumatic fever mitral involvement more common in females aortic valve in males.
Address : Low economic status, over crowed areas is more predisposed to rheumatic fever.
Occupation:
Date of admission :
Chief complaints: Note down the chief complaints in chronological order.
H/o present illness : Expansion of symptoms
1. Dyspnoea:
Ask for
- Onset – sudden (or) gradual in onset
- Duration – how long (represents severity)
- Progression static (or) progressive (reflects the nature of disease).
- Grade – NYHA classification
- Grade I – Dyspnoea on unaccustomed work
- Grade II – Dyspnoea on daily activity
- Grade III – On mild exertion
- Grade IV at rest.
- Aggravating factors – Exercise → exertional dyspnoea ↑dyspnoea on lying down but relieved on sitting → orthopnoea.
- Relieving factors
- Relieved by sitting – orthopnoea
- Relieved by taking rest
- Medications – furosemide, bronchodilators, corticosteroids
- Dyspnoea is of cardiac origin (or) respiratory origin.
- Cardiac origin – Increased burden on heart leads to pulmonary congestion
- Paroxismal nocturnal dyspnoea – person gets up with dyspnoea 2 – 3 hr after going to bed it is seen in LVF.
- Orthopnoea: On lying down, dyspnoea increases. It is decreased by sitting (or) standinSeen in LVF on lying down→ ↑ venous return to heart (already there is left sided failure) ↑ burden heart, which leads to pulmonary congestion. On sitting – diaphragm will be in the dependent area ↑ thoracic volume, lungs can be expanded to the maximum. Also the venous return decreases. So less dyspnoea.
2. Chest pain:
- Site-Right (or) left precordium.
- Character of pain – squeezing, dragging, pricking.
- Radiation – radiation to left arm, forearm, shoulder, back.
It is due to emergence of nerves from same dermatomes (Referred pain). - Onset, duration, progression associated sympathetic symptoms – vomiting, sweating etc.
- Aggravating factors – assessed in terms of grade
- Grade I – Unaccustomed work
- Grade II – accustomed work
- Grade III-on mild exertion
- Grade IV at rest
- Other factors heavy meal, cold air etc.
- Relieving factors
- On taking rest
- On medical therapy – sublingual nitroglycerin.
- It is cardiac (or) respiratory in origin.
- Cardiac origin is usually exertionaRespiratory origin chest pain→ ↑ with inspiration.
- Aorta dissection – sudden chest pain which is of tearing variety radiating to interscapular area.
3. Palpitations:
Abnormal subjective awareness of heart beat.
- Onset sudden (or) gradual; continuous or intermittent
Duration how long - Progression
- Rate
- Rhythm regular (or) irregular
- ↑ by exertion, alcohol;
- Relived by rest.
4. Edema:
- If the edema is generalised ask for where it started first. In right-sided failure edema starts usually in the dependent parts (Pedal edema) then gradually affects other parts.
- Onset, duration, progression.
- Pitting (or) non pitting
- Non pitting edema seen in myxedema.
- Prolonged standing will increase the pedal edema relieved on elevation of legs.
5. Syncope:
- Sudden loss of consciousness
- Onset, duration, progression
- Duration < 1 min usually cardiac > 1 min mostly neurogenic
Syncope Causes:
- Cardiac
- Arrhythmias Brady → Av block sick sinus syndrome
- LV dysfunction
- Aortic stenosis
- Hyper trophic obstructive cardio myopathy.
- Neurogenic – TIA epilepsy
- Metabolic – Hypoglycemia
- Other causes – Vasovagal syncope
- Carotid sinus hypersensitivity
- Postural hypotension.
- Situational cough, micturition, defecation (valsalva), Deglutition.
6. Fatigability:
- Easily get tired
- Fatigue usually due to low cardiac output, ↓ perfusion of tissues and easily tired.
7. Cough with expectoration:
Cough with expectoration Described in respiratory system:
- In LVF, pulmonary edema and consequent infection leads to lower respiratory tract infection.
- Blood stained sputum (hemoptysis) can occur in → mitral stenosis, LVF.
- Ask for – LVF symptoms like PND, Orthopnoea; cough with expectoration; hemoptysis.
- Ask for RVF pedal edema, abdominal fullness (due to hepatomegaly); ascites.
- H/o fever in RHD fever indicates infective endocarditis
- H/o weight loss
- H/o sore throat, joint pains for rheumatic fever.
- H/o hematuria
- H/o pressure symptoms like dysphagia, dyspnoea congestion of face, neck veins H/o Hoarseness of voice
- Due to enlargement of left atrium pressure on recurrent laryngeal nerve – Ortner’s syndrome.
- H/o past illness – any similar complaints in the past attacks rheumatic fever. Known case of DM/HTN/TB (or) CAD.
- Any previous cardiac surgery.
Family history – similar complaints in the family
- DM/HTN/CAD/Contact with TB.
- Alarfan’s syndrome
- Hypertrophic cardiomyopathy
- Prolonged QT syndrome.
Cough with expectoration Personal history:
- Appetite
- Sleep
- Muturition
- Bowel movements
- Habits smoking, alcoholism.
Cough with expectoration Drug history:
- H/o intake of drugs
- Digoxin consumed 5-days/week
- NSAIDS, Antihypertensives
- Penicillin prophylaxis incase of RF.
Cough with expectoration Generation Examination:
- Build and nutrition
- Signs of infective endocarditis – like SWAN OF PEACE
- S: Splenomegaly
- W:Weight loss
- A: Anemia
- N: Nephritis
- () : Osler’s nodes
- F: Fever
- P: Petechiae
- E : Effervescent rash
- A : Arthritis
- C: Clubbing
- E: Embolism
Cough with expectoration Marfan’s features:
- Arm span > Height by > 3 cm
- Upper segment: Lower segment ratio (normal 1.7:1)
- Hyperextension of joints (Pternberg’s thumb sign)
- High arched palate
- Lens dislocation (ectopia lentis) usually superotemporal, low set ears.
Cough with expectoration Vital signs:
- Pallor-seen in infective endocarditis (or) Anemia complicating CC
- Icterus – RVF → Hepatomegaly (Hepatic congestion)
- Cyanosis, clubbing – Infective endocarditis and congenital heart diseas
- Grade of clubbing:
- Grade I – Obliteration of between nail and nail bed
- Grade II – Parrot beak appearance
- Grade III – Drumstick appearance
- Grade IV – Associated with osteoarthropathy.
- Cyanosis
- Central
- Peripheral
Cough with expectoration Central:
Cough with expectoration Cardiac causes:
- Cyanotic congestive heart disease
- AV communications
- Left heart failure.
Cough with expectoration Respiratory causes:
- Pneumonia/COPD
Cough with expectoration Abnormal hemoglobins:
- Sulphhemoglobin and methhemoglobin.
Cough with expectoration Peripheral:
- Exposure to cold
- Raynaud’s disease.
Cough with expectoration Koilonychia:
Cough with expectoration Lymphadenopathy:
- Edema – like in RVF.
Cough with expectoration Vital data:
- Temperature – Raised (or) not
- PR (Pulse Rate)
- Rate – Bradycardia (or) Tachycardia
- Rhythm:
- Irregularly irregular – atrial fibrillation.
- Trigemini, quadrigemini.
- Character – look at carotids
- Volume it denotes left ventricular output
- Normal, high/ AR
- Low / Dehydration; low stroke volume.
- Condition of vessel wall
- In elderly, the vessel is thickened due to arteriosclerosis.
- Any radio radial delay
- Radio femoral delay – coarctation of aorta.
- Blood pressure – Record in both upper limbs, lower limbs and also in supine sitting – positions
- Wide pulse pressure – AR
- Narrow pulse pressure – AS
- Hill’s sign-femoro brachial pressure difference> 20 mm of Hg in AR.
- Respiratory rate count for complete 1 min
- Abdominal (or) Diaphragmatic
- Regular (or) irregular.
Cough with expectoration Inspection:
- Precordium – Any bulging (or) flattening Bulging seen in pericardial effusion is limited only to intercostals spaces.
- Apical impulse – It is seen in the 5th intercostals space 1⁄2 inch medial to mid clavicular line. It is shifted to outward and downward in LVF shifted to outward only RVF. Tapping apex – MS; forcible apex – MR, AR, Anemia; Heaving apex – AS, HTN.
- Other pulsations:
- Arterial: carotids pulsation like dancing carotids (Corrigan sign seen in AR).
Epigastric pulsations – aneurysm of aorta right ventricular hypertrophy; hepatic pulsations in TR/TS
Suprasternal pulsations – Seen in MR, AR - Venous-jugular venous pulse (JVP)
It is seen when the patient lying supported on examiners hand at 450.
It reflects pressure in right atrium.- ‘a’, c, v waves are positive; X and Y are negative
- ‘a’ wave due to atrial systole
- Tin RVH, pulmonary hypertension tricuspid stenosis.
- ‘c’ wave due to backward displacement of tricuspid valv
- ‘v’ wave – due to filling of right atrium
- ‘x’ atrial relaxation.
- ‘y’ as the tricuspid valve opens, pressure in right atrium falls.
- Tricuspid regurgitation – Tc and v waves
- Rapid y descent
- In atrial fibrillation ‘a’ waves are abolished.
- Left parasternal pulsation – it indicates right ventricular hypertrophy. Dilated veins over the flank; any sinuses, scars
- Arterial: carotids pulsation like dancing carotids (Corrigan sign seen in AR).
Cough with expectoration Palpation:
- Apical impulse – Palpate and note down any deviation.
Apical pulse may not be felt in→ pleural, pericardial effusions, obesity, emphysema; when it is behind rib. - Parasternal have – indicate RVH.
- If P2 is palpable in 2nd left intercostals space – pulmonary HTN.
- Thrills – palpable murmur is called thrill.
It indicates grade III of murmur. - Arterial pulsations – palpate in upper limb for – Radial, brachial, carotids in the neck
- Lower limb femoral, popliteal, post tibial, dorsalis paedis.
- Note any femoral delay as in coarctation of aorta.
Cough with expectoration Percussion:
- Left 2nd ICS – If it is dull indicates pulmonary hypertension
- Right 2nd ICS- If it is dull, systemic hypertension.
- Left border- usually in the 5th ICS
- Percussion started in 6th ICS at mid axillary line and is percussed medially till the cardiac dullness felt.
- Right border – not percussable as it is retrosternal
- Upper border – peruses in the left 3rd ICS.
Cough with expectoration Auscultation:
- Mitral area 5th ICS 1⁄2 inch medial to mid clavicular line.
- Auscultate S1 and 2
- Note any split
- Any S3, S4
- Any additional sounds – murmur, clicks, opening snap, pericardial ru
- Murmur – describe as – Timing, Attitude with respiration – ↑ (or) ↓
- Intensity
- Radiation
- Character
- Grade into ‘5’ grades thrill is grade ‘4’.
- Grade 1 faint
- Grade 2- clearly audible
- Snap-MS, TS
- Clicks – AS, PS.
- Pericardial rub – pericarditis.
Example for description of murmur: - MDM in mitral stenosis
- Rough rumbling MDM low pitch, with (or) without opening snap
- Pre systolic accentuation ↑ on expiration better heard in left lateral position, with the bell
- No radiation
- Tricuspid area – four the left ICS near sternal edge
- Examine the same
- Aortic area – second right intercostals space.
- Pulmonic area – second left intercostals space (ICS) near sternal edge.
- Look accentuated (or) diminished P2.
- Accentuated P2 in – Pulm. Hypertension
- Diminished in – pulmonary stenosis.
Cases
Mitral Stenosis:
Name: Anjali
Age: 25 year
Sex: Female
Address: XXXXXXXX
Occupation: Housewife
Chief complaints: Shortness of breath since 9 months
Cough with hemoptysis since 1 month.
H/o present illness:
- Shortness of breath – insidious onset, gradually progressing exertional duration nine months, grade III aggravated by exertion, lying down position
- Relieved by taking rest and sitting position.
- Cough with hemoptysis cough is associated with blood in sputum. It is insidious onset, gradually progressinAsk for quantity of blood (massive (or) blood tinged). Cough is not associated with raise of temperature.
- No H/o chest pain
- No H/o palpitations
- No H/o Swelling of legs
- No H/o syncopal attacks
- No H/o squatting episodes (due to dyspnoea in TOF)
- No H/o fever (to rule out infective endocarditis).
- H/o past illness when she was 16 year old she had migratory type of polyarthritis involving knee, ankle. She also gives the past history of sore throat.
- No H/o medication taken in the past.
- Two days back she got up in the night with dyspnoea.
- Not a known diabetic (or) hypertensive, No H/o contact with TB.
Mitral Stenosis Family history:
- No H/o similar complaints in the family members.
Mitral Stenosis Personal history:
- Appetite – Decreased
- Sleep Disturbed
- Micturition – Normal
- Bowel movements – Normal
- No addictions.
Mitral Stenosis Drug history:
- No H/o drug intake related to this context.
Mitral Stenosis General examination:
- Average built, moderately nourished
- Other signs of RF – like nodule
- Cornea
- Erythema marginatum – not present.
- Signs of infective endocarditis – not present.
- No marfanoid features present.
Mitral Stenosis Vital signs:
- No H/o pallor (PICKLE) not seen.
Mitral Stenosis Vital data:
- Temperature – not raised
- PR-78/mt, low volume, regular, normal character, peripheral pulses palpated equally condition of vessel wall normal.
- BP-100/70 mm of Hg in supine position
- RR-30/mt (normal 18-22/mt)
- Regular, abdomino thoracic.
General Medicine Practicals for Medical Students
Mitral Stenosis Inspection:
- Precordium – No deformity of pericardium.
- Bulging if seen it indicates long duration of disease.
- Apical impulse – it is present in 5th intercostals space 1/2″ medial to mid clavicular lin
- It is tapping type of apex.
- No other pulsations
- Left parasternal haeve seen (it indicates dilated left atrium).
Mitral Stenosis Palpation:
- Apical impulse – It is palpated in the 5th intercostals space 1/2″medial to mid clavicular line.
- Parasternal haeve seen.
- No palpable P2 (It indicates no pulmonary HTN)
- A diastolic thrill palpable in the mitral area best felt in left lateral position and in full expiration.
- Arterial pulsations are felt in upper limb – radial brachial carotids in the nec
- In lower limb femoral, popliteal, post. Tibial A, Dorsalis paedis.
Mitral Stenosis Percussion:
- 2nd left ICS resonant (indicates no pulm. HTN)
- 2nd right ICS-resonant (indicates no systemic HTN)
(No aortic dilatation)
No enlarged cardiac borders.
Mitral Stenosis Ascultation:
- Mitral area – S1 is sharp and accentuated
S2 is audible
Opening snap heard just before S2.
Murmur: low pitched mid diastolic rumbling murmur with presystolic accentuation or grade III intensity. No radiation of murmur. It is best heard with the bell of stethoscope in left lateral position, better during expiration. - No others sound heard.
- Tricuspid area – S1 S2 heard
- Aortic area – S1 S2 heard
- Pulmonic area – S1 S2 heard.
- Examine other system→ nervous, respiratory, GIT (important)
Mitral Stenosis Provisional diagnosis:
- Anatomical-involving mitral valve
- Structural abnormality – stenosis
Mitral Stenosis Etiological:
- Rheumatic
Mitral Stenosis Complications:
- No pulm. HTN,
- No CCR
- No SABE
Mitral Stenosis Rhythm:
- Sinus rhythm.
- Mitral valve stenosis of rheumatic etiology with sinus rhythm and with no other complications.
- The above case is MS with rheumatic etiology because → summarise the positive findings of case and support your diagnosis.
Mitral Stenosis Discussion:
- Loud S1 in MS due to – Loudness of Si depends on – pressure gradient volume gradient across the A-V valve.
In mitral stenosis, due to diastolic pressure gradient; high across the mitral valve Sot he valve is wide open during the whole diastolAs the systole begins, the widely open valve rushes to closIt gives loud sound loud S1.
Seen in – MS, TS, Anemia, thyrotoxicosis, pregnancy, WPW syndrome. - Opening snap – It is produced at the onset of ventricular diastole when mitral valve just about to open.
Mitral Stenosis It represents:
1. Pliable valves
- It is not heard if the valves are calcifie
2. MS is organic
3. Significant MS
4. It can also represent severity of MS.
- Close the opening snap to S2 greater the severity of MS.
5. Presence of opening snap→ Balloon valvuloplasty can be planned
6. Opening snap heard in – MS, TS, ASD, VSD, PDA.
Mechanism of Hemoptysis in MS:
- Pulmonary apoplexy – due to rupture of dilated bronchial (or) pulmonary veins due to left atrial pressure.
- Pulmonary edema occurs in MS due to increased blood flow in pulmonary circulation. It leads to cough with hemoptysis as a result of capillaries rupture and blood poured into the alveoli.
- Any associated bronchitis can cause hemoptysis.
Mechanism of Hemoptysis in MS Mitral facies:
- Peripheral cyanosis of cheeks, tip of nose, lips due to vasoconstriction as a result of low cardiac output in MS.
- Malar flush due to vasodilation over malar region.
Mechanism of Hemoptysis in MS Severity of MS:
- The distance between opening snap and S2 judges severity closer the distance greater the severity.
- Severity of MS assessed indirectly by assessing the severity of pulmonary hypertension.
- Atrial fibrillation and thromboembolic episodes suggest severe MS.
Severity of MS does not depend on intensity and duration of murmur.
The duration of murmur depends upon heart rate.
- Normal mitral valve 4-6 cm².
- Mild 1.5-2.5 cm²
- Moderate-1.1-1.5 cm²
- Severe – <1 cm²
In MS, mid diastolic murmur heard but not complete diastolic murmur. It is because from S2 sound to the opening of mitral valve is the period of isovolumetrirelaxation during there is no blood flow. So no murmur heard in the early diastolic perioMurmur is heard from mid diastole after isovolumetric relaxation is complete.
Mechanism of Hemoptysis in MS Differential diagnosis of MS:
MDM is heard in MS, TS, carey combs murmur (Acute, Rheumatic fever) due to valvulitis.
Audtin flint murmur, left atrial myxoma, ball valve thrombus cortriatrum, ASD, VSD.
Presystolic accentuation of MDM in MS- It is due to last 4 of diastole (between S2-S1) atrial contract, which leads to presystolic accentuation of murmur.
Graham steel murmur – In MS, pulmonary regurgitation to right ventricle leads to early diastolic murmur (EDM) known as graham steel murmur.
Mechanism of Hemoptysis in MS Etiology of MS:
1. Rheumatic heard disease
2. Mucoolysaccharidosis – Type I→ Hurler’s syndrome
Type II → Hunter’s syndrome.
3. Amyloidosis.
4. In elderly due to calcification of mitral valve.
Lutembachar syndrome – ASD (Ostium secundum) along with MS marked cardiomegaly is seen.
Symptoms and signs of MS:
Symptoms and signs of MS Symptoms:
1. Exertional dyspnoea, noctural dyspnoea
2. Cough with hemoptysis
3. Fatigability due to low cardiac output
4. Symptoms secondary to thrombo embolic episodes as a result of dilated left atrium – stroke (CVA) Chest pain
5. Atrial fibrillation can occur→ palpitations (irregular).
Symptoms and signs of MS Signs:
1. Mitral facies
2. Atrial fibrillation
3. Thrombo embolic phenomenon
4. Pulmonary hypertension
- Crepitations
- Pulmonary edema
- Effusion
- Loud P2
5. On ascultation -S, loud opening snap heard MDM with pre systolic accentuation.
Symptoms and signs of MS Investigations:
1. X-ray chest PA view:
- Straight left heart border. Large left atrium indenting on esophagus elevation of left main stem bronchus.
- Signs of pulmonary venous hypertension – edema.
2. ECG:
- Tall ‘p’ waves → represents pulmonary hypertension, left atrial hypertrophy.
- Right ventricular hypertrophy tall ‘R’ waves in V1 V2 V3 deep ‘S’ waves in V4 V5 V6> 35 mm.
- Right axis deviation – negative waves in lead I (L1) positive waves in avF.
3. Echocardiography
- Thickened immobile mitral valves
- Reduced valve area
- Reduced diastolic filling of left ventricle
- Left atrial enlargement.
4. Doppler
- Prolonged pressure half time across mitral valve.
- Evidence of pulmonary hypertension.
5. Cardiac catheterization:
- Pressure gradient noticed across left atrium and left ventricle.
Symptoms and signs of MS Management:
Symptoms and signs of MS Medical management:
- Anticoagulant therapy – as a result of enlarged left atrium, atrial fibrillations lead to thrombo embolic episodes. Warfarin (Vit K antagonist) given as anticoagulant.
- Diuretics frussemide (loop diuretic) given to relieve pulmonary edema.
- Digoxin – In atrial fibrillation to reduce ventricular overload, digoxin is helpfu
- Antibiotic prophylaxis against infective endocarditis.
Surgical management:
Surgical management Indications:
- Uncontrollable pulmonary edema.
- Dyspnoea and intermittent pulm. Edema.
- Evidence of pulm. HTN.
- Recurrent systemic emboli.
Mitral valvotomy (or) commissurotomy – It is effective patients without mitral regurgitation.
Surgical management Balloon valvuloplasty – It is performed in:
- Isolated mitral stenosis with MR
- Mobile non calcified valve
- Left atrium free of thrombus.
Surgical management Mitral valve replacement:
- Very severe MS
- Rigid and calcified valves then replacement surgery indicated replacement using prosthetic valves.
Surgical management Complications of prosthetic valves:
- Thrombosis
- Para valvular leak
- Endocarditis
- Degeneration of biological valves.
Warfarin anticoagulation for atleast three months for biological valves longer periods for mechanical valves.
Anaemia
Name: Neelima
Age: 30 years
Sex: Female
Address: XXXXXX
Occupation: XXXXXXXX
Chief complaints: Loss of appetite and Shortness of breath.
Anaemia H/o present illness:
- Weakness – generally since one week, Loss of appetite since one month.
- Increased irritability and tinnitus.
- Shortness of breath since ten days. Was treated for worm infestation by schisotoma.
Anaemia Family history:
- No H/o similar complaints in the family members.
Anaemia Personal history:
- Appetite – Decreased is a vegetarian.
- Increased bleeding during menstrual cycle.
Anaemia Drug history:
- No H/o drug intake related to this context.
Anaemia General examination:
- Average built, ill nourished
- No signs of jaundice.
Anaemia Vital signs:
- Pallor is seen.
Anaemia Vital data:
- Temperature – not raised
- PR-90/ min, low volume, regular, normal character, peripheral pulses palpated equally condition of vessel wall normal
- BP-140/70 mm of Hg in supine position
- RR-25 min.
Anaemia Inspection:
- Apical impulse – it is present in 5th intercostals space 1⁄2″ medial to mid clavicular linIt is tapping type of apex.
Anaemia Palpation:
- Apical impulse – It is palpated in the 5th intercostals space /1⁄2″medial to mid clavicular line.
- Arterial pulsations are felt in upper limb – radial brachial carotids in the necIn lower limb – femoral, popliteal, post. Tibial A, Dorsalis paedis.
Anaemia Percussion:
- 2nd left ICS-resonant (indicates no pulm. HTN)
- 2nd right ICS-resonant (indicates no systemic HTN)
(No aortic dilatation)
No enlarged cardiac borders.
Anaemia Auscultation:
- Mitral area – Normal
- Tricuspid area – Normal
- Aortic area – Normal
- Pulmonic area – Normal
- Examine other system→ nervous, respiratory, GIT (important)
Provisional diagnosis – Anaemia:
Anaemia Investigations:
- MCV decreased (Normal = 77-93fl)
- MCH decreased (Normal = 27-32 Pg)
- MCHC decreased (Normal = 30-35 g/dl) Serum ferritin – decreased
- Haemoglobin-7gm/dl.
Anaemia Final diagnosis:
- Iron deficiency anaemia
Anaemia Treatment:
- Ferrous sulphate 200 mg/day increased diet rich in iron.
- In severe cases iron dextran is given i m or iv.
Tricuspid Stenosis
Etiology:
- Rheumatic heart disease
- Carcinoid syndrome
Tricuspid Stenosis Clinical features:
1. Symptoms:
- Symptoms of right heart failure – Pedal edema fatiguability, Abdominal swelling, Hepatic discomfort (Jaundice).
2. In inspection:
- Giant’a’ waves seen in jugular venous pulse.
- Apex impulse may be shifted outward representing right heart failur
3. On palpation:
- Mid diastolic thrill felt at the lower sternal border in tricuspid area.
- Pre systolic pulsations of liver palpable.
On palpation Tricuspid Stenosis Ascultation:
- S1 loud
- MDM, low pitch murmur, increasing on inspiration, better heard with the bell of stethoscope, heard in the tricuspid area.
On palpation Tricuspid Stenosis Investigations:
- Chest radiograph – enlarged right atrium seen.
- ECG-Tall, peaked ‘p’ waves, normal axis.
- Echocardiography – (M-mode) – Tricuspid valve thickening decreased early diastolic filling sloe pf the tricuspid valve. Mitral valve also usually abnormal.
- 2D Echo – enlarged right atrium.
- Doppler – prolonged pressure gradient across tricuspid valve.
- Cardiac catheterization – it is the diagnostic.
On palpation Tricuspid Stenosis Management:
- Tricuspid valvotomy.
- Balloon valvuloplasty.
- Valve replacement therapy.
Mitral Regurgitation
Etiology:
- Rheumatic heart disease.
- Mitral valve prolapse (Myxomatous degeneration of valve) – floppy mitral valve
- Papillary muscle dysfunction.
- In Myocardial infarction papillary muscle rupture can occur.
- Rupture of chordac tendinae.
- Infective endocarditis – damage to valve cusps.
- Cardiac tumors – left atrial myxoma.
Etiology Mitral Regurgitation Clinical features:
1. Symptoms
- Pulmonary edema
- Dyspnoea, orthopnoea
- PND
- Nocturnal dyspnoea
- Crepitations are represent left ventricular failure.
- Palpitations.
- Fatigability – due to low cardiac output.
- Symptoms of right heart failure
- Pedd edema
- Abdominal full ness
- Hepatic discomfort.
2. On inspection:
- Prominent and hyper dynamic apical impulse seen lateral to the mid clavicular line and downward below 5th ICS representing enlarged left ventricle.
- Precordium maybe bulged.
3. On palpation:
- Apex impulse forceful and brisk.
- Systolic thrill palpable in apical area, which is best palpable in left lateral position and during expiration.
- Left parasternal haeve present (due to RVH).
- P2 may be palpable in left 2nd ICS (Diastolic shock) representing pulmonary hypertension.
4. Ascultation:
- S1 may be normal (or) muffled due to pan systolic murmur.
- Prominent S3 (due to LVF).
- Atrial fibrillation – irregular beat.
- Murmur – A high-pitched, soft blowing pan systolic murmur, which is heard best with the diaphragm of stethoscope and during expiration. Murmur radiates to left axilla, inferior angle of scapula.
5. Examine other systems:
- GIT→ Liver may be enlarged
- If severe ascites may be present.
- Respiratory system:
- Vesicular breath sounds
- Crepitations may be heard during pulmonary edema
- Nervous system examination.
6. Assessment of severity of MR:
- S3 (third heart sound) when heard it is severe.
- Presence of mid diastolic murmur.
- Degree of left ventricular hypertrophy.
- Intensity of the murmur
- Soft S1.
7. Investigations:
- Chest X-ray – enlarged left ventricle, left atrium.
- ECG – Left axis deviation
- Left ventricular hypertrophy
- ‘P’ waves broad, tall
- Echocardiogram (M-mode)
- Thickened mitral valve
- Vegetation over the leaf let seen.
- Enlarged left ventricle may be with low function.
- 2D Echo: Same as above but the information is reliable.
8. Doppler:
- Regurgitation flow into left atrium noted.
- Evidence of pulm. Hypertension.
Mitral Regurgitation Management:
1. Medical management:
- Diuretics to relieve pulmonary edema.
- Vasodilators – like ACE inhibitors, Ca2+ channel blockers.
- Digoxin may be prescribed if atrial fibrillation is present.
- Anticoagulation therapy incase of atrial fibrillation.
- Antibiotic prophylaxis against infective endocarditis.
2. Surgical management:
- Intra aortic balloon counter pulsations – reduce regurgitation flow by decreasing peripheral vascular resistance.
- Indications for surgery:
- Refractory conditions to medical therapy.
- Ejection fraction < 55-60% (normal 65%).
- End systolic ventricular dimension > 4.5/5 cm on echo valve repair in surgery of choicNow a day’s thoracoscopic procedure is available.
Tricuspid Regurgitation
Tricuspid Regurgitation Etiology:
- Rheumatic heart disease.
- Isolated TR seen in intravenous drug abscess (Infective endocarditis).
- Ebstein’s anomaly.
4. Secondary to:
- Function TR – due to right ventricular dilatation.
- Right ventricular infarction.
- Pulmonary hypertension.
Tricuspid Regurgitation Clinical features:
1. Symptoms:
- Fatigability
- Pedal edema
- Abdominal fullness
- Hepatic discomfort.
2. On inspection:
- Large ‘V’ wave seen in JVP
- Rapid Y descent.
3. On palpation:
- Right ventricular pulsations.
- Liver pulsations in right upper quadrant.
- Systolic thrill may be palpable occasionally.
4. Ascultation:
- Atrial fibrillations may be present.
- A pan systolic murmur heard in tricuspid and is better heard during inspiration.
5. Investigations:
- X-ray enlarged right atrium and ventricle.
- ECG – Right axis deviation
- Left ventricular hypertrophy.
- Echocardiogram (2D) – Tricuspid valve thickening decreased early diastolic filling.
- Doppler – prolonged pressure half time across tricuspid valve.
Tricuspid Regurgitation Management:
- Underlying cause treated – treat the mitral valve disease (or) other left sided lesions.
- Valvuloplasty is preferred to valvular replacement.
Aortic Stenosis
Aortic Stenosis Etiology:
- Rheumatic heart disease.
- Bicuspid aortic valve (congenital) – can cause AS
- Calcification of aortic valve in elderly.
- Familial hypercholesterolemia
- Mucopolysaccharidoses
- Aortic valve area 3-4 cm2
- <0.8 cm2 severe stenosis.
- Mucopolysaccharidoses
5. Function As
- In anemia
- Thyrotoxicosis
- Severe AR.
Aortic Stenosis Clinical features:
1. Symptoms:
- Exertional dyspnoea
- Angina
- Exertional syncope
- Pulmonary edema – crepitations sudden death can occur.
2. On inspection:
- Apex (heaving type)
3. On palpation:
- Power heaving apex
- In left ventricular enlargement – Apex outward, downward displacement.
- Systolic thrill may be palpable over aortic area.
- Small and slowly raising carotid pulse.
4. Auscultation:
- Ejection click heard.
- A harsh mid systolic ejection murmur with radiation to carotids.
- It is best heard in expiration with patient sitting and leaning forward and with diaphragm of stethoscope.
- Ejection click
- It is heard due to sudden opening of aortic (or) pulmonary valve.
- It represents that the stenosis at the valvular level and the stenosis is milder degree.
- Mid systolic murmur
- Usually pressure gradient between left ventricle and aorta is the greatest during middle of systolSo in as the murmur is mid systolic ejection murmur.
Aortic Stenosis Types of valvular stenosis (AS):
- Valvular stenosis – at the level of valve.
- Supra valvular – Vitamin D intoxication, William syndrome.
- Elfin facies – seen in William’s syndrome – low set ears, hypertelorism, broad forehead, pointed chin, upturned nose, folded upper lip.
- Sub-valvular stenosis – below the level of aortic valve.
- Idiopathic hypertrophic subaortic stenosis (IHSS) (or) Hypertrophic obstructive cardiomyopathy (HOCM).
- Fibro muscular subaortic valvular stenosis.
5. Investigations:
- X-ray Concentric left ventricular hypertrophy Prominent ascending aorta.
- ECG – left ventricular hypertrophy.
- Echocardiogram (2D) – Thick aortic valve.
Left ventricular hypertrophy.
Post stenostic dilatation of aorta. - Doppler – Increased transvalvular velocity.
- Cardiac catheterization – the diagnostic.
6. Management:
- Medical management: Management of left heart failure as described earlier.
- Surgical management:
- Indications:
- Severe left ventricular hypertrophy.
- Pressure gradient between left ventricle, aorta > 80 mm of Hg.
- Aortic valve area < 0.8 cm2.
- Indications:
- Valve replacement:
- By using bio prosthetics (or) Mechanical valves.
Aortic Stenosis Ross procedure:
- Patient’s pulmonary valve replaced onto aortic valve and bioprosthetics used for pulmonary valve on right sidAs bioprosthetics are better taken up on right side.
Aortic Regurgitation
Etiology:
- Congenital bicuspid valve.
- Rheumatic heart disease
- Marfan’s syndrome
- Atheroma, syphilis, ankylosing spondylitis.
- Infective endocarditis.
Aortic Regurgitation Clinical features:
1. Symptoms
- Palpitations
- Angina
- LVF – Exertional dyspnoea
- Orthopnoea
- PND
- Nocturnal dyspnoea.
2. On inspection
- Hyper dynamic apex
- Apex may be displaced outward and downward Suprasternal pulsations seen.
3. On palpation – Various signs of AR
- Quincke’s sign – visible capillary pulsations of finger nails.
- Locomotor brachialis – High bounding brachial pulse.
- Corrigan’s sign – dancing carotids.
- De Musset’s sign – Head nodding along with carotid pulsations.
- Water hammer pulse-collapsing pulse (high volume).
- Durozeiz murmur – Diastolic murmur heard when the femoral artery is compressed distally.
- Systolic murmur when compressed proximally.
- Traube’s sign – Pistol shot sounds heard over the femoral artery with stethoscope.
- Hill’s sign – usually he difference between systolic BP of lower limb is 20 mm of Hg
- Useful in assessment of severity of AR
- Mild – 20-40 mm of Hg.
- Moderate-40-60 mm of Hg.
- Severe -> 60 mm of Hg difference
- Wide pulse pressure seen in AR.
- Pulsations of uvula – Muller’s sign.
- Ladolfi’s sign – Change of size of pupil with each cardiac systole.
- Light house sign – Alternate flushing and blanching of forehea
- Diastolic thrill may be palpable in aortic area.
NCERT General Medicine Practical Notes
Aortic Regurgitation Ascultation:
- Reduced A2 sound
- High-pitched soft blowing early diastolic decrescendo murmur best heard in sitting, leaning forward, in full expiration with diaphragm of stethoscopMurmur best heard at the neoaortic area.
4. Investigations:
- X-ray – Moderate to severe left ventricular enlargement prominent aortic knuckle.
- ECG – Left ventricular hypertrophy.
- Echocardiogram (2D)
- Diastolic vibrations of the anterior leaf let of mitral valve.
- Early closure of mitral valve.
- Dilated left ventricle.
- Doppler Demonstrates dilatation.
5. Management:
- Manage left ventricular failure as described above.
- Aortic valve replacement in those with
- Severe symptoms
- Ejection fraction < 50%.
Aortic Regurgitation Zones criteria for rheumatic fever:
1. Major criteria
- Carditis
- Migratory poly arthritis
- Chorea
- Erythema marginatum
- Subcutaneous nodules.
2. Minor criteria
- Fever
- Arthralgia.
- Previous rheumatic fever
- Raised ESR, CRP
- Prolonged PR interval
- First (or) second degree AV block.
- For the diagnosis of RF – 2 major criteria (or) 1 major = 2 minor criteria required.
Aortic Regurgitation Infective Endocarditis:
Aortic Regurgitation Swan Of Peace
- S: Splenomegaly
- W: Weight loss
- A: Arthritis
- N: Nephritis.
- O: Oster’s nodes
- F: Fever
- P: Petechiae
- E: Effervescent rash
- A: Anemia
- C: Clubbing
- E: Echymosis.
Aortic Regurgitation Investigation for SABE:
- CBP→ pallar leucocytosis
- ESR raised
- Blood culture – to isolate organism
- CVE- hematuria, proteinuria
- ECG – PR interval prolonged AV block
- 2D ECHO-vegetations > 2 mm detected.
- Trans esophageal echo (TEE) vegetations <2 mm can also detected.
Aortic Regurgitation Diseases predisposing to endocarditis:
- Valvular heart disease – MR, AR, VSD, PDA, Bicuspid aortic valve, TOF, Prosthetic heart values.
Aortic Regurgitation Continuous Murmur:
- It is seen in PDA
- Aorto-pulmonary fistula
- Ruptured sinus of valsalva.
Respiratory System
Case Proforma:
Name:
Age:
Sex:
Address:
Occupation:
Date of admission:
Chief complaints: Note down the chief complaints in chronological order
H/o present illness – describe the complaints
1. Cough:
- Insidious onset (or) sudden onset
- sudden onset represents – foreign body inhalation, acute allergy, acute infection.
- Duration of cough – Recent (or) prolonged duration.
- Progression Progressing (or) not (represents severity of disease)
- Productive (or) Dry
- Dry cough – Upper respiratory tract infection
- Early tuberculosis
- Croup (laryngo tracheo bronchilis) – brassy cough
- If productive describe the sputum.
Respiratory System Sputum:
- Quantity of sputum – large (or) scanty
- Large amount of sputum seen in -Bronchiectasis; lung abscess
- Scanty sputum – chr. bronchitis.
- Colour of sputum
- Yellow→ purulent
- Pink frothy-hemoptysis (MS, LVF)
- Rusty colour – pneumococcus, pneumonia
- Greenish blue -pseudomonas
- Red current jelly – klebsiella pneumonia
- White – mucoid sputum (Chr. Bronchitis upper respiratory tract infections)
- Brown color – anchovy saule pus (Amoebic abscess).
- Consistency-thick (or) thin
- Thick and sticky sputum – Chr. Bronchitis, URTI, br. Asthma.
- Smell whether it is foul smelling (or) not
- Foul smelling sputum
- Lung abscess
- Bronchiectasis
- Broncho pleural fistula
- Infections
- Foul smelling sputum
- Appearance of sputum
- Mucoid sputum
- Chr. Bronchitis
- Br. Asthma.
- Upper respiratory infections
- Mucoid sputum is very thick and sticky.
- Mucopurulent – indicates bacterial infection.
- Serous water like → left heart failure, Broncho alveolar ca.
- Mucoid sputum
- Hemoptysis
- Streaks of blood along with sputum
- Onset, duration, progression, quantity of blood coughed up. Massive hemoptysis – TB, Bronchiectasis, lung abscess, rupture of bronchial (or) pulmonary artery (> 100-600 ml/day)
Respiratory System Time:
- Morning, soon after getting up from bed – represents Bronchiectasis, Lung abscess.
- Cough in early hours of morning with associated dyspnoea seen in – br. Asthma, LVF.
- More during night time – usually paroxysmal cough as laryngo tracheo bronchitis more common during night seen in→ pertussis, br.
- Asthma, left ventricular failure.
Respiratory System Seasonal:
- Cough more during winter and morning time
- COPD (chronic obstructive pulmonary disease) Chr. Bronchitis, emphysema.
Respiratory System Postural variation:
- Increased cough when diseased lung is dependent cough decreased when the diseased lung in higher position (cough increased when the person sleep to the side of diseased lung) → seen in Bronchiectasis; Lung abscess
- In pleural effusion, cough may be relieved if sleep towards diseased lun
- In supine position, more cough seen in brassy cough due to compression of trachea, bronchi by mediastinum.
2. Breathlessness:
- Onset – gradual (or) sudden
- Sudden onset
- Foreign body aspiration
- Pneumothorax
- Pulmonary infarction
- Empyema
Increased cough, after ceasation of cough ↑ dyspnoea: Pneumothorax.
- Duration – How long
- Progression (or) not (to know the severity)
- Grade of dyspnoea – already described in CVS
- Paroxysmal – bronchial asthma
- Dyspnoea on exposure to allergen (or) any change of weather (cold) → br. Asthma.
- Dyspnoea associated with chest pain; fever – pleural effusion.
- Dyspnoea of respiratory origin is not exertional present at rest also.
- Breathlessness may be continuous
- → COPD
- Interstitial lung disease
- Breathlessness may be continuous
3. Chest pain:
- Ask for site
- Character
- Radiation referred along intercostals nerves
- Associated with exertion (or) not
- Associated with cough, respiration.
- Chest pain of respiratory origin (usually pleuritic) is not exertiona
- It is increased with inspiration. Associated with cough (mild), fever.
- Pleuritic pain aggravated by inspiration, cough.
- If the person sleeps towards the side of pleurity – chest pain relieved
- Pain is referred along the intercostals nerves.
4. Fever:
- Onset sudden (or) gradual
- Duration – how long
- Progression-fever progressing (or) relieved
- Type of fever
- Continuous fever-fever is continuously above normal and the fluctuation less (<10 C). Does not touch baseline.
- Example: Enteric fever (typhoid)
- Pleurisy, rheumatic fever, meningococcal meningitis miliary tuberculosis. Remittent fever – fever is always above normal but the fluctuation is large (> 20 C) and never touches baseline.
- Example: Amoebic liver abscess
- Acute bronchopneumonia Septicaemia
- UTI.
- Continuous fever-fever is continuously above normal and the fluctuation less (<10 C). Does not touch baseline.
- Intermittent fever – fever present for few hours and it touches baseline during sometime of the day. (gap of 24 hr)
- Quotidian – daily raise and daily fall.
- Example: UTI, TB, pus any where in the body.
- Double infection p. vivax.
- Tertian alternate day fever (gap between paroxysms is 48 hr)
- Benign tertian → p. vivax, p. ovale.
- Malignant tertian – P. falciparum.
- Quartan – fever comes after every two days. (a gap of 72 hr present between paroxysms) e.P. malariae
- Double quotidian – double fever spike in a single day (same day – raise, fall both seen)
- Example: Kala-azar
- Gonococcal endocarditis
- Military tuberculosis.
- Quotidian – daily raise and daily fall.
- Relapsing fever – fever upto 40° for a few days then followed by a febrile period (may even upto a week)
- Example: Pel-ebsein fever – Hodgkin’s lymphoma.
- Grade of fever – Low grade (or) high grade.
- Low grade fever – Tuberculosis (not above 38° C)
- In TB fever is low grade and evening rise; night sweats.
Respiratory System Associated with chilli and rigors:
- Malaria
- Filaria
- UTI/Pyelonephritis
- Pus any where
- Kala-azar
Associated herpes labialis – vesicles caused by simplex seen on lips (angles) during high fevers.
- Seen in → Pneumonia
- Malaria
- Meningitis
- Severe streptococcal infection.
Respiratory System Diurnal variation:
- Evening rise of temperature with night sweats – Tuberculosis
- Usually fever is more during night time due to cireadian rhythm of steroids (less during night time).
- For 1º C raise of temperature, pulse raises by 10.
- Fever is associated with tachycardia except typhoid fever, viral fever.
Respiratory System Ask for negative history:
Any H/o jaundice (seen in – pulmonary infarction military TB; Cor pulmonale
Respiratory System CVS symptoms:
- H/o Fatigability
- H/o Syncopal attack
- H/o PND, orthopnoea
- H/o palpitations
Respiratory System Corpulmonale (right heart failure occurs):
- H/o Pedal edema
- H/o Distension of abdomen
- H/o Jaundice.
H/o Past illness – Any H/o TB, Br. Asthma, any similar complaints in the pass any H/o of contact with TB known DM/HTN (Routine history).
Respiratory System Family history:
- Ask for any similar complaints in family members.
- Any H/o contact with TB (among family members)
Familial conditions – Heritable – cystic fibrosis, a anti trypsis deficiency
- Any H/o atopy (Allergic)
Personal H/o- appetite
Sleep
Micturition, Bowel movements
Addictions – smoking in pack years – no. of packs/day x no. of years of smoking
Respiratory System Drug history:
- Any intake of aspirin which causes asthma (Drug induced).
- Mechanism – aspirin inhibits prostaglandin synthesis.
- So compensatory ↑ production of leukotrienes leading to bronchial asthma (bronchospasm).
- Prostaglandin usage – Aggravates asthma
- Non selective ẞ blockers – Asthma ↑ (bronchoconstriction)
Respiratory System General examination:
- Built/Nutrition
- Patient is conscious/coherent/comfortable.
- Examine spine – any kyphosis, scoliosis
- Measurements spinoscapular distance, AP diameter; transverse diameter hemithorax diameter.
Respiratory System Vital signs:
Respiratory System Pickle:
- Examine
- Cyanosis, clubbing, koilonyehia described in spotters
Respiratory System Vital data:
- Temperature
- PR
- BP
- RR-Rate count for complete 1 min.
- Rhythm-regular (or) irregular.
- Character – abdominal (or) thoracic
- Thoracic – abdominal movement less seen in – Diaphragmatic palsy
- Peritonitis
- Severe ascitis
Abdominal – thoracic movements less seen in – pleurisy
Collapse of lung.
Respiratory System Systemic examination:
- Upper respiratory tract
- Nose; sinuses (look for sinus tenderness)
- Oral cavity – look for tonsillitis
- Pharynx – inspect the post pharyngeal wall – for infection, nodules.
- Lower respiratory tract
- Inspection
- Shape of chest:
- Normally – chest is bilateral symmetrical Elliptical in shape.
- AP diameter < transverse diameter (5 : 7 ratio) Intercostals spaces broader infront than behind
- Shape of chest:
- Inspection
Respiratory System Deformities:
1. Pectus excavatum (cobbler’s chest) – funnel chest
- Depression of sternum compared to ribs
- Severe cases – Dysphagia (due to compression of esophagus)
- Palpitations.
2. Pectus carinatum (Pigeon chest)
- Protrusion of sternum
- Seen in rickets (or) congenital deformity.
3. Barrel chest – Barrel like
- AP diameter of chest > transverse diameter
- Intercostals spaces widened
- Seen in – emphysema.
4. Flat chest
- Thoracic case is long and narrow due to reduced AP diameter.
- Due to bilateral fibrosis of lungs.
Respiratory System Asymmetry:
- Kyphosis – bending of spine forward with convexity backwards
- Severe cases
- Pulmonary hypertension
- Right heart failure
- Severe cases
- Scoliosis Lateral bending of spine.
- Kyphoscoliosis – Combination of Kyphosis and Scoliosis.
- Lordosis Back bending of spine with concavity backwards.
Respiratory System Respiratory movements:
2. Rhythm – Regular (or) Irregular.
Respiratory System Irregular respiration:
- Chyne stokes breathing – Waxing and waning of respiration (Hypernoea and apnoea alternating).
- Causes Opium, Barbiturate poisoning
- LVF
- Damage to cerebral hemisphere and diencephalons
- Uremia
- Deep sleep
- Cardio respiratory embarrassment.
- Biot’s breathing – irregularly irregular respiration.
- Causes meningitis
- ↑ ICT
- Kusmual breathing – Rapid and deep respiration.
- Causes – Diabetic ketoacidosis
- Uremia
- Starvation ketoacidosis.
3. Type of breathing
- Normal breathing is abdomino thoracic
- Normal in females – thoraco abdominal
- Thoracic breathing – ↓ abdominal movements seen in diaphragmatic palsy, peritonitis.
- Abdominal breathing-thoracic movements seen in pleuricy, collapse of lung.
4. Movement of chest wall
- Usually both sides of chest wall move uniformly.
1. Unilateral diminished movements
- Pleural effusion
- Consolidation
- Hydro pneumothorax
- Massive collapse
- Fibrosis of lung
- Obstruction of main bronchus.
2. Bilateral diminished movements
- Emphysema
- Bronchial asthma
- Bilateral fibrosis, consolidation.
- Look any retraction (or) fullness of intercostals spaces
- Retractions (or) chest in drawing seen in labooured breathing as in severe pneumonia, COPD
- Intercostals full ness seen in – empyema.
Respiratory System Mediastinum:
Look whether mediastinum is central (or) deviated
- Trail sign – Sterno mastoid tendon becomes prominent on the side of tracheal deviation (by inspection only).
- Look for deviation of any apical impulse.
→ Shift to same side of pathology- Collapse
- Fibrosis
- Pleural thickening.
Respiratory System Shift to opposite side of pathology:
- Pleural effusion
- Pneumothorax
- Hydropneumothorax.
Respiratory System Central in position:
- Consolidation
- Interstitial lung disease
- Bronchiectasis
- Emphysema
- Lung abscess.
Look for any drooping of shoulder:
- It is seen in
- On the same side
- Fibrosis of lung
- Collapse of lung
- On the same side
Respiratory System Spino scapular distance:
- On inspection, spino scapular distance on both sides compared.
- Decreased in – fibrosis collapse on same side.
Respiratory System Look for sinuses, scar, pulsation, engorged veins:
Respiratory System Palpation:
Inspectory findings are confirmed by palpation.
- Shape of chest wall
- Respiratory movements.
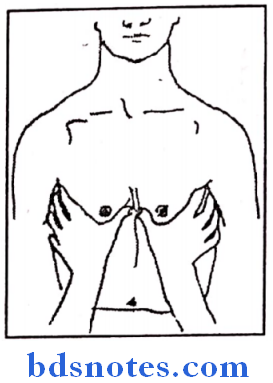
1. Movements of upper lobes:
- Hands are placed in such a way that, fingers present over the trapezius muscle and the thumbs are stretched infraclavicularly to meet in mid line.
- Patient is asked to take breathing → after inspiration Thumbs are moved apart.
- If respiratory movements – thumb movement equal Decreased movements on that side thumb movement decreased → Thumbs are present at irregular distance from mild line.
2. Movements of middle lobe
- Right side – middle lobe
- Left side – lingual
- Hands are placed in such away that fingers present in axillary region (at 5th, 6th intercostals spaces) and thumbs inframmarily placed and are stretched to meet in midline at the midsternal linPatient asked to take breathinAfter inspiration, distance between thumbs compared to assess the respiratory movements.
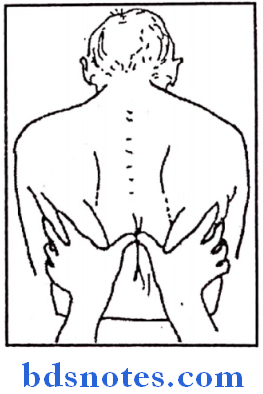
3. Movements of lower lobe
- Seen on posterior aspect of chest walHands are placed infrascapularly finger place below scapula and the thumbs stretched to meet in midline.
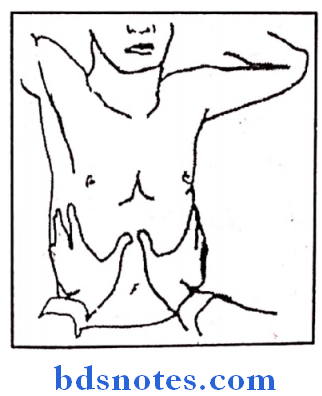
4. Movements of diaphragm:
- Patient will be in supine position, hands are placed at the lower ribs (costal margins) in such away that thumbs meet in midline at xiphisternum.
- Distance between thumbs is interpreted to assess the movements of diaphragm.
Respiratory System Deviation of mediastinum:
1. Position of trachea
Patient is asked to extend his neck, index finger, ring finger of right hand placed over sterno clavicular joints and the middle is used to palpate the trachea to follow the whole course of trache. At the end, distance between fingers on sterno clavicular joints and the trachea noted compared on both sides. Decreased distance on one side represents tracheal deviation to that side
2. Apex beat – apex beat palpated to know its position
- Whether deviated (or) not.
- Normal apex – In 5th ICS 1/2 “medial to mid clavicular line.
Deviation of mediastinum Look sinus tenderness:
- Maxillary sinuses – over maxillary bone
- Frontal sinus – over superonasal part of orbit on its medial wall.
Deviation of mediastinum Tactile vocal fremitus (TVF):
Patient is asked to speak “one, two; one, two”. Then with the ulnar border of hand chest wall palpated on both sides to compared the vocal fremitus.
Deviation of mediastinum Mechanism:
Spoken word causes sound vibration, which travel along the larynx, bronchi, and then lung parenchyma, which causes vibration of chest wall.
Deviation of mediastinum TVF decreased in:
- Pleural effusion
- Pneumothorax
- Hydropneumothorax
- Bronchial asthma
- Lung fibrosis
- Lung collapse due to distal bronchial obstruction
- Emphysema
Deviation of mediastinum TVF increased in:
- Consolidation
- Following pulmonary infarction
- Cavitation
- Collapse due to peripheral bronchial obstruction.
Deviation of mediastinum Look for local tenderness over intercostals spaces:
- They are tender in empyema.
Deviation of mediastinum Measurements:
- Measure
- Spino scapular distance
- AP diameter
- Transverse diameter
- Chest circumference – Inspiration and expiration – (5 cm difference should be present).
- Hemithorax diameter.
- In emphysema – AP diameter > transverse diameter > 5:7
- Spinoscapular distance – Fibrosis and collapse of lun
- Hemithorax decreased – fibrosis and collapse.
Deviation of mediastinum Percussion:
Rules of percussion:
- Left middle finger that is placed over intercostals space – plexymeter
- Right middle finger with which percussed – plexor
- Plexor and plexymeter should be perpendicular to each other
- Percussion movement should involve from only at the wrist
- Percussion started
- From resonant to dull area
- From normal side to pathological side.
1. Impaired note
- Consolidation (Woody note)
- Fibrosis, Collapse
2. Dull note
- Pleural thickening.
3. Stony dull
- Pleural effusion
- Solid intrathoracic tumor
4. Tympanic note (Drum like resonance)
- Pneumothorax, emphysema, superficial cavity.
5. Skodiac resonance (Sub tympany)
- Boxy quality resonance
- Seen in relaxed lung above the level of pleural effusion.
6. Hyper resonance:
- Pneumothorax
- Emphysema
- Large cavity
- Eventration of diaphragm.
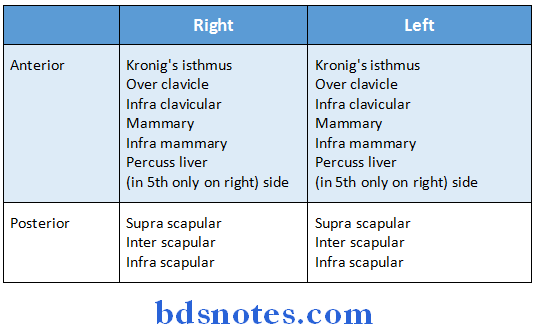
Hyper resonance Kronig’s isthmus:
Band of resonance of 5-7 cm width
- Bound medially by neck muscle
- Laterally by – shoulder muscles
- Anteriorly clavicle
- Posteriorly trapezius
- Decreased note (width) – apical lobe fibrosis (TB)
- Increased width of resonance- emphysema
Hyper resonance Liver dullness:
Liver percussed from 5th ICS in mid clavicular line down until the resonant note over abdomen appears and this length noted which represents liver span.
Hyper resonance Liver dullness may even start from above (4th ICS):
- Collapse of lung.
- Fibrosis of lung
Hyper resonance Liver is pushed down and the dullness may not be noted in 5th ICS:
- Emphysema
- Pneumothorax
Tidal percussion – liver border in 5th ICS percuss in mid clavicular line during inspiration and expiration.
During inspiration – Liver is pushed down and the 5th ICS will be resonant If it is dull → then fibrosis of lung – basal lobe.
Shifting dullness
- It is useful in hydro pneumothorax
- In upright (sitting) position
- Hyperresonant note above (air)
- Dull note below (fluid).
- In supine position
- Shifting dullness seen
- Dull note above.
Hyper resonance Auscultation:
Auscultation Breath sounds:
Auscultation Types:
1. Vesicular – Long inspiration (Tubular phase, alveolar phase)
- Short expiration
- Without any gap between the two
- Normal breath sounds are vesicular (Rustling type)
- Tubular phase
- Alveolar phase
- Expiration
2. Bronchial sounds – These are heard over trachea, bronchi.
Alveolar phase absent. So inspiration expiration but with a gap in between. As alveolar phase absent, no rustling quality; bronchial sounds are hollow in character.
Auscultation Types of bronchial breath sounds:
- Tubular – High pitched – consolidation; above the level of pleural effusion cavity.
- Cavernous – low pitched, as though blowing into empty bottle heard over cavity.
- Amphoric-metallic quality – Heard over – smooth walled cavity; open pneumothorax.
3. Broncho vesicular sounds:
- Inspiration – Both tubular, alveolar phase present Expiration – prolonged due to resistance No gap between the two.
- Heard in Bronchial asthma
- Chr. Bronchitis
- Emphysema.
- Breath sounds are diminished in→ collapse fibrosis
- Absent in
- Pleural effusion
- Empyema
- Pneumothorax
- Hydropneumothorax.
Auscultation Adventitions sounds:
1. Rales – They are considered to be bubbling sound due to entry of air into fluid. Types coarse rales, medium, fine rales (or) Crepitations. Fine rales are heard (due to fluid in alveoli) heard in
- Heard at the end of inspiration.
- LVF
- Pulmonary edema
- Tuberculosis.
- Pneumonia.
Medium rales (smaller bronchi involved)
- Heard in mid inspiration
- Bronchiectasis.
Coarse rales (large bronchi involved)
- Heard in initial inspiration
- Chronic bronchitis.
Post tussive rales
- Heard during inspiration following coug
- Due to minimal pathology in alveoli.
2. Rhonchi
- Ascultatable wheeze is rhonchi
- They represent continuous musical sound.
- Polyphonic (sonorous) – expiratory musical sound contains several notes of different pitch.
- Monophonic – Single musical note heard due to spasm of single airway. Heard in end of expiration, heard in – bronchitis emphysema.
Auscultation Causes:
- Bronchial asthma
- COPD
- Localized obstruction
- Tropical pulmonary eosinophila
- Cardiac failure.
- In bronchial asthma sound are – Polyphonic rales sibilant (involvement of smaller airways).
Stridor – Loud inspiratory sound due to airway obstruction (usually upper) (larynx trachea)
Auscultation Pleural rub:
- It is due to rubbing two inflamed pleura.
- It is heard end of inspiration (or) starting of expiration
- Usually heard in basal parts of lung.
- They are accentuated, pressure of chest piece over chest wall increased.
- Not altered by coughing.
- Associated with pain, tenderness.
- Seen in – pleuricy.
Succussion splash – In hydropneumothorax, on shaking the patient a splashing sound produced.
- Post tussive suction – It is heard after coughing in smooth walled cavity.
- During cough air expelled from cavity
- After cough, during inspiration-air sucked in
Vocal resonance – when person asked to speak ‘one two, one two’ vocal vibration produced in larynx are carried down trachea, bronchi, bronchiole, lung parenchyma, chest wall.
→So any intervening fluid, air→ decreased vocal fremitus.
→Consolidation lung parenchyma – ↑ vocal fremitus. Vocal fremitus (or) absent
- Pleural effusion
- Pneumothorax
- Pleural thickening
- Emphysema.
↑ in- Cavity
- Consolidation
- Fibrosis.
Auscultation Types:
1. Bronchophony – Sounds are loud and clear but words cannot be made out.
- Seen consolidation.
2. Egophony – Nasal quality of sound heard when auscultated
- Seen – above level of pleural effusion; above pneumothorax.
3. Whispering pectoriloguy – Individual words can be made out
Auscultation Causes:
- Consolidation
- Cavity.
Cases
Pleural Effusion:
Auscultation Chief complaints:
- Dry cough
- Fever
- Chest pain
- Breathlessness (Dyspnoea)
Pleural Effusion On inspection:
- Diminished respiratory movements on affected side.
- Apical impulse may be shifted to opposite side.
- Trachea deviated to opposite side as evidenced by prominent sternomastoid tendon on shifted side (trail’s sign).
- There may be fullness of intercostals spares on affected side.
Pleural EffusionOn palpation:
- Confirm the above inspectory findings.
- Tactile vocal fremitus – decreased on affected side.
- Usually no tenderness elicited in intercostals spaces unless empyema present.
Pleural Effusion Percussion:
- Percussion started from normal to pathology side
- There is stony dullness noted on percussion on the affected side.
- If it is only pleural effusion no shifting dullness elicited.
Pleural Effusion Auscultation:
- Diminished breath sounds on the affected side.
- Vocal resonance diminished on affected side.
- Pleural rub may be heard over basal part of lung on affected sidJust above the level of pleural effusion – tubular breath sounds, bronchophony, whispering pectoriloquy may be heard.
Pleural Effusion Diagnosis:
- Right/left sided
- Pleural effusion of tuberculous etiology/malignancy/some other etiology.
Pleural Effusion Discussion:
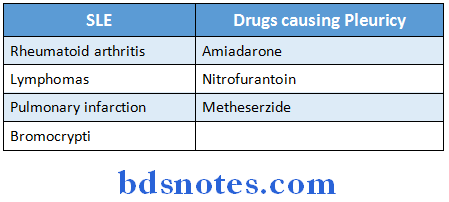
- Etiology
- Exudative
- Tuberculosis
- Pneumonia
- Rheumatoid arthritis, SLE
- Bronchogenic carcinoma
- Pancreatitis
- Pleural mesothelioma
- Pulmonary infarction
- Exudative
Pleural Effusion Meig’s syndrome:
Pleural Effusion Some may consider it exudative and others transudative:
- Fibroma of ovary pleural effusion
- Ascites
Pleural Effusion Transudative:
- Congestive cardiac failure (prominent right sided effusion)
- Nephritic syndrome
- Cirrhosis of liver
- Hypothyroidism
- Hypoproteinemia (Protein losing enteropathy, severe hepatic disease, nephritic syndrome).
Difference between exudative and transudative pleural effusion:
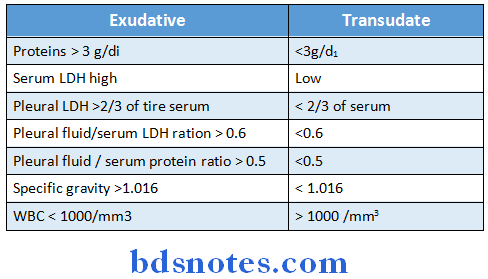
Pleural LDH >2/3 of the serum < 2/3 of serum
Pleural fluid/serum LDH ration > 0.6′ < 0.6
Pleural fluid/serum protein ratio > 0.5 < 0.5 these three constitute Light’s criterion
- Pleural fluid LDH, Pleural fluid/Serum LDH, protein ration – Light’s criterion.
- In pleural effusion due to →
1. TB
- Lymphocytes predominate in pleural fluid
- Positive mycosacterium on AFB stain Pleural fluid usually amber coloure
- Raised ADA (Adenine deaminase) levels.
- PCR can be used to detect bacteria.
2. Malignancy
- Serous (or) blood stained fluid.
- Malignant cells may
- be seen.
- Pleural biopsy can detect malignancy.
3. Rheumatoid arthritis
- Serous pleural fluid
- Usually lymphocytes predominate glucose levels of pleural fluid very low.
4. SLE
- Serous fluid
- Lymphocytes can be seen
- ANA seen (anti Ds DNA)
5. Acute pancreatitis
- Serous (or) Blood stained fluid
- Raised amylase in pleural fluid
- Predominal left sided.
- Raised amylase in pleural fluid seen in esophageal perforation also. It is predominant left sided effusion.
Pleural Effusion Normal pleural fluid:
- Normal fluid is 5-15 ml
- 200 ml pleural fluid should be collected for radiological diagnosis 75 ml-100 ml fluid is enough to diagnose it on lateral decubitus view on X-ray.
- CT scan detects as little as 10 ml of fluid.
- 500 ml of fluid should be accumulated for clinical manifestation.
Pleural Effusion Chylous pleural effusion:
- Milky pleural fluid
- Pleural fluid show increased triglyceride levels (>100 mg/dl)
Pleural Effusion Causes:
- Tuberculosis
- Thoracic outlet obstruction (malignancy)
- Trauma
- Filariasis
- Lymphoma
- Hypothyroidism.
Pleural Effusion Bilateral pleural efusion:
Pleural Effusion Investigations:
Pleural Effusion Routine:
- CBP
- RBS CVE (Proteinuria seen in Nephrotic syndrome)
- ESR BI.Urea
Pleural Effusion Specific:
- X-ray chest PA view – It shows obliteration of costophrenic angle.
- X-ray lateral view – It is useful to differentiate pleural effusion from consolidation.
- Lateral decubitus view – detects 75-100 ml of fluid also.
- Pleural fluid tapped and sent for analysis.
- Cytology
- Gram stain/AFB stain
- Amylase (Pancreatitis, esophageal perforation)
- ADA levels (TB)
- Proteins LDH (to know exudative (or) Transudate)
- Culture of the pleural fluid.
- Pleural biopsy to confirm malignancy.
- CT scan – For loculated pleural effusion
- To know any malignancy.
- Manteaux test (for TB)
- Bronchoscopic guided biopsy (for malignancy when suspected mass detected) (Transbronchial biopsy).
Pleural Effusion Management
- Incase transudative pleural effusion, primary lesion is corrected. (or) exudativ(ATT for TB etc), Bed rest, good nutrition.
- Thoracocentesis (or) Pleural fluid aspiration
- Done in case of – Severe respiratory distress
- Massive fluid (or) Rapid collection of fluid.
- Tube thoracostomy – Intercostal tube placed to drain the fluid
- Place of intercostals tube usually 5th ICS anterior to mid axillary line
- Triangle of safety Anterior border of lattismus dorsi
- Posterior border of pectoralis major
- Superior border of 5th rib.
4. In recurrent pleural effusion due to malignancy pleurodecis performed by using:
- Tetracycline, doxycycline
- Tale (asbestos free)
- Bleanycine, carmustine
- Corynebacterium paruum
- Kaolin.
5. In case of parapneumonic effusion- due to pneumonia.
- If pH between 7.2-7.3, LDH => 1000 U/ml – Pleural fluid aspiration.
- Pleural fluid pH <7.2 glucose < 60 mg/dl – Tube thoractomy.
- When pleural effusion uncomplicated it is relieved by antibiotics.
6. Empyema
- Etiology – Secondary infection of hemothorax
- Rupture of lung abscess, rupture of subphrenic abscess Rupture of tuberculous cavity
- Any penetrating injury
- Septicaemia.
Empyema Features:
- Patient is toxic – high grade fever with rigors tachycardia
- Inter costal fullness, tenderness present
- Overlying skin may be inflamed
- Empyema necessitantis – some cases pus collected below skin which is communicating with pleural cavity in empyemIt shows cough impulse (expansile on cough).
Empyema Investigations:
- X-ray chest PA view – usually not distinguished from pleural effusion
- Aspiration of pus from pleural cavity – sent for culture and sensitivity.
Empyema Investigations Management:
Empyema Non tuberculous empyema:
- When pus is thin drained by intercostals tube
- When thick – Intercostals tube flushed with 20 ml normal saline 6 hrly. Streptokinase may be inserted daily for 3 days.
- In chronic cases – if no previous aspiration then resent empyema sac (parietal pleura)
- When previous aspiration done – then decortication (visceral pleural also removed)
Empyema Investigations Tuberculous empyema
- ATT started
- Pus is aspirated using wide bore needle.
Pulmonary Fibrosis (Localized)
- Movements of chest wall slightly reduced on the side of lesion.
- Mediastinal shift seen towards the lesion.
- Trail’s sign – sternomastoid tendon prominent on side to which trachea deviated (usually towards the lesion).
- Percussion – Impaired note is noticed.
- Breath sounds – low-pitched bronchial breath sound heard.
- Coarse crepitation may be heard (coarse rales).
Cavitation
- Movements of chest wall reduced on side affected.
- There may not be mediastinal shift. But when it is associated with fibrosis shift towards lesion.
- Percussion – Impaired note heard.
- Breath sounds – (Bronchial breathing).
- Heart in cavity
- Tubular breathing
- Cavernous breathing
- Amphoric breathing heard over smooth walled cavity.
- Heart in cavity
- Vocal resonance – Increased
- Whispering pectorilogy – individual words can be made out heard
- Other sounds – coarse rales.
Collapse Of Lung
Collapse due to obstruction of major bronchus:
- Reduced chest wall movements on the affected side.
- Mediastinal shift towards the lesion.
- Percussion note – usually dull.
- Breath sounds – diminished (or) absent.
- Vocal resonance – Reduced (or) absent.
- Usually no adventitions sounds heard.
Collapse due to obstruction of peripheral bronchi:
- Reduced chest wall movements on affected side
- Mediastinal shift towards lesion
- Percussion note – dull
- Breath sounds – high pitched bronchial breathing.
- Vocal resonance – increased and whispering pectorilogy heard.
- Adventitious sounds – may be absent (or) sometimes coarse rales heard.
Copd (Emphysema)
- Movements of chest wall and symmetrically diminished on both sides.
- Usually no mediastinal shift.
- Percussion note – Hyper resonant
- Kronig’s isthmus – Increased width of resonance band
- Liver dullness – may not be elicited in 5th ICS. It is still resonant not dul
- Breath sounds – Vesicular sounds but diminished prolonged expiratory phase.
- Vocal resonance – It may be normal (or) reduced.
- Adventitious sounds – Ronchi (expiratory) heard.
Copd (Emphysema) Investigations:
- X-ray chest
- Hyperinflation of lung fields
- Widened intercostal spaces
- Diaphragm is flattened.
- Pulmonary function tests:
- Represents COPD
- FEV1/FEC ratio – <70%.
- FEV1 < 80%
- Total lung capacity, residual volume increased.
- CT scan can detect extent of emphysema.
- α1 antitrypsin levels – In congenital absence of α1 AT leads to pan acinar emphysema.
Copd (Emphysema) Management:
- Stop smoking, and exposure to smoky dust avoided.
- Bronchodilators – B2 agonists like salbutamol (Inhalation)
- Steroids Inhalation of steroiIt halts the inflammatory process.
- Incase of infection – Appropriate antibiotic therapy used.
- Long-term low concentration of oxygen delivered to the patient gives good results.
- Surgical excision – young patients, severe disease (or) a, AT deficiency – done.
Consolidation
- Chest wall movements reduced on the affected side.
- No mediastinal shift.
- Percussion note – may be impaired note.
- Breath sounds – High pitched tubular breath sounds heard over the region of consolidation.
- Vocal resonance
- Increased
- Whispering pectorilogy – heard.
- Adventitious sounds – Fine rales are heard.
- Organisms causing pneumonia
- Pneumococcus
- Chlamydia pneumoniae
- Mycoplasma pneumoniae
- Legionella influenza
- Klebsiella pneumonia – Involves upper lobes
- Coxiella burnetti.
- Atypical pneumonia – chlamydia, Mycoplasma, coxiell
Consolidation Community acquired pneumonia:
- Pneumonia that occurs outside hospital (or) diagnosed within 48 hr after hospital admission in a patient who has not received long term care for 14 days (or) more.
Hospital acquired pneumonia – Pneumonia developing> 48 hr of hospital admission.
- If the patient is on H2 blockers → pH of gastric acid increase
- It facilitates microbial growth, which may predispose to pneumonia.
- If Sucralfate given – no TpH so no pneumonia.
Consolidation Investigations:
- X-ray chest PA view – It shows opacity in the lung fields.
- Air bronchogram in the lesion also suggests consolidation.
- Sputum Sent for gram stain / AFB.
- Culture and sensitivity.
- Arterial blood gas analysis – In severe pneumonia ↓ PO2,↓ PCO2.
- Routine CBP (Leucocystosis), ESR.
- Monteaux test for TB.
Consolidation Management:
- Oxygen therapy (>30% conc.)
2. Antibiotic therapy:
- Chlamydia – Erythromycin (or) tetracycline
- Klebsiella – Gentamycin (or) Amikacin + Ciprofloxacin (or) +third generation cephalosporin.
- influenza – Azithromycin.
- Mycoplasma – Clarithromycin (or) Azithromycin.
- Legionella – Erythromycin (or) clarithromycin.
- Pneumococcus – Ampicillin
- Ampicillin + clavulanic acid.
Consolidation Complications of pneumonia:
- Parapneumonic effusion
- Pneumothorax
- Empyema
- Lung abscess
- Dissemination of infection.
Pneumothorax
- Reduced (or) absent chest wall movements on affected side
- Mediastinal shift towards opposite side.
- Percussion note – hyper resonant
- Breath sounds – Diminished (or) absent (Sometimes bronchial breathing).
- Vocal resonance – Reduced (or) absent.
- Adventitious sounds – usually rales heard when fluid also present.
- Coin test – coin placed on affected side and percussed with another coin, metallic sound can be heard with stethoscope.
Pneumothorax Types of pneumothorax:
Pneumothorax Spontaneous pneumothorax:
- Due to Rupture of emphysema bulla, pleural bleb
- Rupture of sub-pleural TB focus
- Pulmonary infarction
- Bronchogenic carcinoma.
- Closed air entered the pleurBut no the bronchopleural fistula closeBreathlessness seen but is mild.
- Open Broncho pleural fistula is still patient. Air freely circulates between pleura and bronchi.
Tension pneumothorax – Valvular communication between pleura and bronchAir enters the pleural but does not leave.
Pneumothorax It is an emergency condition:
- Severe dyspnoea.
- Cyanosis Hypotension.
Pneumothorax Investigations:
- X-ray chest PA view – It shows a line of hypertransluscency which separates collapsed less transluscent lung.
- Film usually taken in expiratory phase.
- Arterial blood gas analysis
- In left sided pneumothorax – Produces ARS axis and T wave change.
Pneumothorax Management:
Pneumothorax Depends on severity:
- Small, stable pneumothorax (Spontaneous_< 15% of hemithorax observation alone may be appropriate.
- 1.5% per day resolution and gets resolved in 10days.
- Usually chest X-ray taken 6 hr later and confirmed that it is progressing.
- Small, but mildly symptomatic – Administration of high flow oxygen the resultant nitrogen gradient will speed the resorption.
- Larger than (>15-20%) symptomatic – Small thoracostomy over a needle (No. 8 Fr) aspirated.
- Those with secondary spontaneous pneumothorax
Pneumothorax Intercostal tube (34-36 Fr):
- Severe pneumothorax
- Tension pneumothorax
Tube thoracostomy (Intercostal tube) inserted and it is placed under water seal.
Hydro Pneumothorax
Hydro Pneumothorax Etiology:
- Secondary infection of open pneumothorax.
- Intragenic conversion of pleural effusion into hydro pneumothorax while aspiration.
Hydro Pneumothorax Features:
- Reduced chest wall movements on the affected side.
- Mediastinum shifted to opposite side.
3. Percussion:
- Horizontal fluid level noticed by dull note (where as in pleural effusion ellis ‘S’ shaped curve)
- Shifting dullness – as mentioned in proforma.
4. Breath sounds – diminished breath sounds.
5. Vocal resonance – reduced.
6. Succussion splash heared on auscultation.
Nervous System
Case Proforma
Name:
Age:
Sex:
Address:
Occupation:
Date of admission:
Chief complaints : Inability to move upper limb and lower limb of one side
: Inability to speak
: Deviation of mouth to one side
H/o present illness: Describe the chief complaints in chronological order. Ask for negative H/o Motor, sensory, cerebellar symptoms, CVS symptoms. (Described in the CVA case)
H/o past illness: Any H/o diabetes, Rheumatic heart disease, Ischaemic heart disease, TIA (transient ischaemic attack), Tuberculosis, asthm:→ Recover within 24 hr
Any previous hemiplegic attacks: RIND recovers in a period of 1 wee(Reversible ischaemic neuronal deficit).
Family history: Any similar complaints in the family
: H/o dyslipoproteinemias.
Personal history:
Diet:
Appetite Sleep:
Micturition:
Bowel movements:
Addiction’s:
Drug history : Ask for smoking
:H/o anti-platelet drugs usage in the past for previous stroke.
Nervous System General Examination:
- Built/Nutrition
- Conscious/Coherent/Comfortable – Mention this
- Attitude of the patient – How is his posture.
- Incase of hemiplegia → upper limb flexor dominate (so flexed)
- Lower limb in extended position describe
Nervous System Skull and spine:
- Skull-Dolicocephalic, Mesocephalic, Brachycephaly;
- Spine- scoliosis, Kyphosis, Lordosis
- Any neurocutaneous markers →→ By looking at certain cutaneous lesion. We can suspect intracranial pathology.
- Café-au-lait spots – brown coloured macules.
- Six (or) more café-au-lait spots >5 mm before puberty
- > 15 mm after puberty.
- Suggestive of neurofibromatosis.
- They are seen in both neurofibromatosis type I and type II
- Type I (Chr-17)→ associated with Lisch nodules in cornea
- Optic nerve glioma
- Axonal freckles.
- Type II (Chr-22)→ associated with
- Schwannoma
- Ependymoma
- Meningioma.
- Ash-leaf-spots; Sha-green patches; Adenoma sebacium → these are all seen in tuberous sclerosis. It is associated with cortical tubers.
- Any haemangiomas → seen in sturge-weber-syndrome – cutaneous, retinal haemangiomas, Rail rod calcification in brain.
- Any hypo-pigmentation, thickened nerves – as in leprosy.
Nervous System Vital signs:
Nervous System Pickle:
- P: Pallor
- I: Icterus
- C: Cyanosis, Clubbing K: Koilanychia
- L: Lymphadenopathy
- E: Edema
Nervous System Vital data:
- Temperature
- PR
- BP
- RR.
Nervous System Systemic Examination:
1. Intellectual functions
- Consciousness – Whether he is conscious or not.
- Rapid loss of consciousness – Intracranial haemorrhage
- Infective (encephalitis meningitis)
- Toxic (Poisonings).
- Behaviour – Ask patient/or attendants
- Whether he is agitated (or) calm
- Any loss of speech.
- Emotional state – Any signs of happiness
- Distress
- Depression
- Depersonalization.
- Any lack of sleep (or) hypersomnia.
- Delusions, hallucination, Illusions
- Delusion- A false belief that cannot be wiped off, even we prove that it is fals(There is no external stimulus).
- Paranoid delusion – somebody killing (attacking) him.
- Delusion of grandenoir – I am rich (elated).
- Nihilistic – The world and I are not existing.
- Hypochondriacal – though the person is healthy, he fells that there is some illness.
- Delusion- A false belief that cannot be wiped off, even we prove that it is fals(There is no external stimulus).
Nervous System Hallucination:
- False perception when no external stimulus existin
- Tactile hallucination – There is something crawling over body.
- Olfactory – even there is nothing, he feels some smell.
- Gustatory – he fells some taste, though nothing is present.
- Illusion – False interpretation of somethinExternal stimulus is present.
- Example: Mistaking snake for a rope.
- Orientation orientation in time, place noted.
- Ask for – what is the time now?
- Where he at this moment?
- Orientation orientation in time, place noted.
Nervous System Memory:
Nervous System Check for:
- Immediate recall
- Recent memory
- Remote memory.
1. Immediate recall – Ask him to repeat what you asked just now?
2. Recent memory – ask him what he had for dinner last night?
3. Remote memory – events that occurred long ago?
- In dementia, organic amnestic syndromes – recent memory, remote memory are lost but immediate recall is sustained.
- In delirium – Immediate recall, recent memory lost but remote memory present.
- Wernicke – Korsakoff syndrome – a type of dementia due to alcohol consumption. (Thiamine deficiency).
- Wernicke’s → confusion, ophthalmoplegia, ataxia, nystagmus
- Lesion is in- mamillary bodies.
- Korsakoff’s syndrome – anterograde, retrograde amnesia and confabulation (filling of memory gaps).
- Intelligence – ask for simple calculations
- Released reflexes – In some conditions, certain reflexes which are kept inhibited arreleased leading to their manifestation.
- They are seen in dementia and confusional state
- In large frontal lobe lesions – grasp reflex is released
- Other released reflexes – Glabellar tap reflex – parkinsonism
- Palmomental reflexes
- Avoiding reflexes – lesions of contralateral parietal lobe
- Snout response
- Suckling reflexes.
Nervous System Speech and language:
- Look for any dysarthria (or) aphasia.
- Dysarthria – Disarticulation of speech
- Cerebellar dysarthria – scanning speech (Scanning a line of poetry) Slurring, impaired timing and coherence.
- Spastic dysarthria (Pseudobulbar) – seen in extra pyramidal lesions.
- Individual syllables are slurred and the precision of consonant pronunciation is lost (Indistinct, breathy mumbling).
- Bulbar – Non specific slurring of speech (Indistinct, slurred, nasal) associated dysphagia, diplopia, ataxia present.
- Parakinsonian – Indistinct, rapid, stammering, quiet.
- Myopathic – Indistinct, poor articulation.
- Aphasia
- Sensory aphasia – Wernicke’s aphasiLesion in the Wernicke’s area of interpretation (posterior parietal cortex).
- Person can see a written word (or) hear an uttered word but cannot interpret the meaning, so don’t know what to speak (Fluent aphasia with poor comprehension and repetition).
- Motor aphasia – Broca aphasia – lesion in Broca’s area (area 44) (in the lower, inferior frontal cortex) written (or) uttered word is interpreted but the signals to the muscles of speech are not sent by Broca are(Non fluent aphasia with good comprehension and repetition).
- Conduction aphasia – Lesion in arcuate fasciculus that connects
Wernicke’s and Broca’s are(Fluent aphasia with good comprehension and repetition). - Global aphasia – When there is extensive lesion involving large areas of speech.
- Speech
- No comprehension
- No repetition
- Non-fluent
2. Cranial nerves:
- Olfactory nerve – Sensory cells in the olfactory epithelium pass via cribriform plate to the olfactory bulFrom here second order neurons start, which go to uncus and para hippocampal gyrus.
- Test for smell using – oil of cloves, peppermint, asafetida
- Common bed side soap, slunt, fruits.
- Anosmia – Lack of sensing smell.
- Parosmia altered sensation of smell.
- Optic nerve-Optic nerve (from ganglion cells) → optic chiasma → optic tract → lateral geniculate body-optic radiation → occipital cortex (17, 18, 19)
Cranial nerves Tests:
- Visual acuity → It is tested by using snellen’s chart for farvision.
Jauger’s chart for near vision.
Incase of illiterates – Landlot’s broken ring chart used. - Visual field – it is tested by confrontation method.
To test patient’s right eye, ask the patient to cover his left eye and look into the left eye of yours. Cover your right eye and look into patient’s right eye.
Cranial nerves By using your finger test:
- Superior field
- Inferior field
- Nasal field
- Temporal field
- Note down any abnormality
- Visual field can also be tested by perimetry.
- Colour vision by ishihara charts.
Cranial nerves Lesions of optic nerve pathway:
- Optic nerve – Ipsilateral blindness
- Optic chiasma – Bitemporal hemianopia
- Pupillary reflex lost (direct)
- Optic tract- homonymous hemianopia
(Wernicke’s hemianopic pupil) - Optic radiation – homonymous hemianopia
- Optic tract- homonymous hemianopia
- Visual cortex – Homonymous hemianopia with macular sparing –
- Pupillary reflex normal.
Cranial nerves Occulomotor (III Nerve), Trochlear IV Nerve, Abduscent-VI Nerve):
- Occulomotor nerve lesions – leads to ptosis (paralysis of levator palpebrae superioris)
- Mydriasis
- Diplopia (Due to extraoccular muscle palsy)
- Loss of pupillary reflex (direct) – Pupil does not constrict on the side of lesion but pupil constrict on the other side (Indirect papillary reflex present).
- Trochlear nerve – It supplies – superior oblique muscle (SO4)
- Superior oblique – main action → intortion
- Accessory → abduction
- Downward movement.
- Abducent nerve:
- It supplies – Lateral rectus (LR6)
- Lateral rectus action – abduction
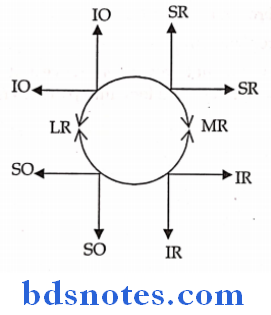
- SR – Superior Rectus MR Medial Rectus
- LR-Lateral Rectus
- IO- Inferior Oblique
- LR-Lateral Rectus
- SO-Superior Oblique.
Except lateral rectus, superior oblique muscle is supplied by occulomotor nerve.
Cranial nerves Gaze palsies:
- Lateral conjugate gaze palsy – lesions of PPRF (Para pontine reticular formation).
- Palsies of conjugate upward gaze – lesions of central parts of mid brain, Inferior thalamus.
- Impaired downward gaze – lower brain stem gaze.
- In cerebral lesions – patient gaze is towards the lesion In brain stem lesions – gaze is opposite to the lesion In epilepsy – gaze is opposite to the lesion.
Cranial nerves Trigeminal nerve (Vth NERVE):
- Fibres from gassarian ganglion enters the lateral surface of pons → bulbospinal tract → spinal cord.
- It is divided into:
- Ophthalmic nerve
- Maxillary nerve
- Mandibular nerve.
- Vth nerve is sensory to face
- Motor to masticatory muscles
- To test the nerve – check for sensations over face
- In trigeminal N. palsy → mandible deviated to paralysed side.
Cranial nerves Facial nerve (VIIth Nerve):
- Facial nucleus (pons) → Facial collicullus → internal auditory canal → middle ear →sternomastoid foramen → divider into peripheral branches.
Cranial nerves Facial nerve branches:
- Greater superficial petrosal → supplies lacrimal and salivary glands.
- Stapedial branch – supplies stapedial muscle.
- Chorda tympanic – sensory to anterior 2/3 of tongue (carries taste sensations).
- Peripheral branches
- Temporal
- Zygomatic
- Buccal – Upper and lower
- Mandibular
- Cervical.
- Facial nerve supplies muscles of expression
Cranial nerves To test the nerve:
- Ask him to close eyes as tightly as possible and look for the tone of orbicularis occuli.
- Ask him to clench his teeth
- In facial N. palsy months deviated to the normal side.
Facial nerve palsy: it is two types
- Supranuclear palsy – Lesion above the facial nucleus; upper part of face of is spared due to bilateral representation in the cortex. Lower part of face is paralysed.
- Taste sensations are not affected
- No atrophy of facial muscles (UMN lesion).
- It is commonly seen in CVA.
- Infra nuclear palsy:
- Bell’s palsy – most common
- Lesion below facial nucleus
- Whole the face (on one side) paralysed
- Month deviated to normal side
- Cannot whistle, no puffing, no closing of lid
- Loss of taste over anterior 2/3 of tongue
- Atrophy of facial muscles.
Cranial nerves Vestibulo – Cochlear nerve – (VIII N.):
- Spiral ganglion → cochlear nucleus, Vestibular nucleus → lateral lemniscus → medial geniculate body → auditory cortex (temporal lobe areas 21, 22).
Cranial nerves Test for cochlear division:
When he is due to hear (or) not
- Rinne’s test – vibrating tuning fork kept over the mastoid,
When the person ceases to hear then placed opposite to meatus. Usually air conduction > (ac) bone conduction (bc) Rinne’s test +ve when ac>bc→ normal ear; sensorineural deafness.- -ve test when bc> ac→ Conductive deafness.
- False -ve Rinne – Unilateral sensorineural deafness.
- Weber’s test:
- Vibrating tuning fork placed over the middle of forehead.
- It is lateralised to worse ear – conductive deafness
- Lateralised to better ear – sensorineural deafness.
- Vibrating tuning fork placed over the middle of forehead.
- Schwabach’s test – compared to that of examiner.
- To test vestibular fibres – caloric test is done
- Water of temperature 37 ± 7° C poured into the meatus look for Nystagmus
- COWS – Cold water opposite side; warm water same side Nystagmus.
- To test vestibular fibres – caloric test is done
Cranial nerves Glossopharyngeal nerve (IX N.):
- It supplies tonsillar fossa.
- Soft, heard palate
- Oropharynx.
It carries both taste and general sensation of post 1/3 of tongue.
Cranial nerves To test the nerve:
- Look for taste sensations
- Palatal reflex – back of pharynx tickled, and note any contraction of palate.
Cranial nerves Vagus nerve (X N.):
Cranial nerves Vagus nerve (X N.) It supplies:
- Soft palate except tensor palati
- Laryngeal muscles
- Pharyngeal muscle.
Cranial nerves Vagus nerve (X N.) Tested by:
- In case of X N. palsy uvula deviated to normal side.
- Gag reflex-Posterior pharyngeal wall stroked look for vomiting reflex.
Cranial nerves Spinal accessory nerve XI N.:
- It supplies – Tapezius
- Sterno cleido mastoid.
Cranial nerves Spinal accessory nerve XI N To test:
- Ask him to shrug the shoulder (action of trapezius)
- In sterno mastoid palsy – Torticollis to the side of palsy.
Cranial nerves Hypoglossal nerve XII N:
- It supplies muscles of tongue except palatoglossus supplied by (X nerve).
Cranial nerves Hypoglossal nerve XII N To test the nerve:
- Movements of tongue
- In XII N. palsy tongue is deviated to the paralysed side.
- Bulbar palsy (LMN) – tongue wasted
- Pseudo bulbar (UMN) – tongue thick
3. Motor system:
- Bulk of muscle – By inspection and palpation bulk noted
- Any atrophy, hypertrophy noted.
- Right – left
- Tone of muscle – Look for tone in muscles hypotony, Hypertoni
- Right – Left
- General Medicine
- Hold the limbs at various joints and move them passively to note the tone of muscles.
- Note the tone of muscles.
- Upper limbs
- Flexors arm, forearm, wrist
- Extensors same.
- Lower limb
- Flexors – thighs, leg, foot
- Extensors same.
- Hypotonia-seen in cerebellar lesions
- Chorea
- Myopathies
- Myasthenia gravis
- Polyneuritis
- Neuronal shock.
- Hypertonia – Rigidity, Spasticity.
- Clasp knife spasticity → resistance appears initially, later on no resistance Seen in UMN lesions.
Motor system Rigidity:
- Cog. Wheel rigidity → Rigidity present at stretches (intermittent)
- Lead pipe rigidity → rigidity seen through out the movement.
- Both are seen in extra pyramidal lesions.
- In basal ganglia lesions (Parkinsonism) rigidity seen.
- Movement and strength – right – Left side
Motor system Test for strength of muscles of upper limb:
- Biceps ask the person to flexion the elbow against resistance.
- Triceps extend the elbow against the resistance.
- Brachiordialis – In mid prone position, ask the person to flex the elbow against resistance.
- Lumbricals
- They cause extension of IP joints
- Flexion of metacarpo phalangeal joints.
- Its paralysis leads to claw hand.
- Interrossei
- Pad – palmar interrossei – adduction
- Dab Dorsal interrossei – abduction
- Palmar interrossei – Card test – Ask the person the hold the card tightly and assess the strength.
- Dorsal interrossei – Egawa test – ask the person to move the middle finger laterally on both directions.
- Serratons anterior – Ask the person push against the wall winging of scapula seen on paralysed side. Trunk Inability to sit up from bed in supine position.
Motor system Lower limb:
- Flexor of knee – semi membranous (semi tendinous, biceps femoris – ask him to flex against resistance).
- Extension of knee – quadriceps – test against resistance
- Flexors of Hip – Iliopsoas.
- Extensors of Hip – Hamstrings.
Motor system Grading of strength:
- 0 – Complete paralysis
- 1 – A flicking type of contractions
- 2 – When gravity excluded, power detected
- 3 – Against gravity
- 4 – against resistance, but some weakness
Grade 5 – Normal strength
Motor system Reflexes:
Motor system Three types:
- Deep tendon reflexes
- Superficial reflexes
- Sphincteric reflexes.
Motor system Deep tendon reflexes:
Principle muscle stretch reflex – when the tendon is stroked, muscle is stretched, muscle spindle is activated, signals reach the spinal cord via, la and II fibres, from the spinal cord efferent impulses reach the muscle spindle through Aẞ (or) Ay – efferents leading to muscle contraction.
It is a monosynaptic reflex.
1. Knee jerk – Knee is flexed, and stroked over the patellar tendon just below the patellIt causes extension of the knee.
- Root value L2 L3 L4
2. Ankle reflex – Foot is slightly dorsiflexed and the stroke given over the Achille’s tendon. Contractions of gastroenemius noted.
- Root value S1 S2
3. Triceps reflex- elbow flexed, forearm rested over the patient’s chest just above the olecranon stroke given to the triceps tendon.
- Root value C7 C8
4. Biceps reflex – Elbow flexed to right angle, finger placed over the biceps tendon and stroke given.
- Root value – C5 C6.
5. Supinator jerk – A stroke given over the styloid process of radius (lower end f radius 4-5 cm above wrist).
Result in contraction of brachio radialis flexion of elbow
Contraction of biceps – flexion of elbow.
- Root value – C5 C6.
6. Jaw jerk – Asked to open the mouth slightly, a finger placed over the chin and gently tappeSlight upward jerk with contraction of muscles of jaw noteIt is brisk in pseudo bulbar palsy.
Motor system Grading of reflexes:
- 0- Absent
- 1- Present (Like the ankle jerk)
- 2- Brisk (like knee jerk)
- 3- Very brisk
- 4 – Clonus.
- In UMN palsy – DTR (Deep tendon reflexes) exaggerated
- In LMN palsy – DTR absent
- In lambert eaton syndrome, frederich’s ataxia – DTR absent.
Motor system Superficial reflexes:
1. Corneal reflex – with a cotton wisp, cornea is tonched from the lateral side; the response is bilateral blinking of eyes.
- Reflex pathway – Afferent nerve – Trigeminal nerve (V N.)
- Efferent nerve-Facial nerve (VII N.).
- Lesions – V N. (Trigeminal) lesions – bilated blinking seen when the elicited eye is normaNo response in either eye seen if the elicited eye is abnormal (Trigeminal palsy).
- VII N. lesion – In VII N. lesions, no blinking of eye on paralysed sid
2. Conjunctival reflex – It is similar to cornea reflex but the conjunctive is touche
- Reflex path way – Afferent nerve – Trigeminal nerve
- Efferent nerve-Facial nerve.
3. Gag reflex (Pharyngeal reflex) – When the posterior wall of pharynx is touched, vomiting sensation occurs.
- Afferent nerve – Glossopharyngeal nerve (IX N.)
- Efferent nerve-X-XI (Vagus, accessory nerves).
4. Palatal reflex – When soft palate is touched, the arch of soft palate gets elevated.
- Afferent nerve-IX N.
- Efferent nerve – X, XIN.
5. Abdominal reflex – with a blunt object abdominal wall stroked from periphery to center around umbilicus you can see the contraction of abdominal muscles and umbilicus drawn to the same side.
- Upper abdomen T8 , T9 (both afferent, efferent)
- Umbilicus – T10
- Lower abdomen – T11, T12 (both afferent, efferent)
- → In UMN lesions abdominal reflex absent initially, later on the reflex returns.
- In LMN lesion, no return of reflex.
- Abdominal reflex may not be elicitable (or absent) – fat abdomen, → following abdominal surgery, when there is rigidity.
6. Cremasteric reflex:
Upper medial 1/3 of thigh on inner side is stroked from above, downwards and also inside – it leads to contraction of cremaster muscle, which shows elevation of testis on that particular side.
- Root value – L1.
7. Anal reflex – When the skin around the anal region is stroked, it leads to contraction of external and sphincter.
- Root value-S3, S4 (S5).
8. Plantar reflex – The limb is flexed at the knee, patient lying position, thigh is externally rotateLateral plantar aspect is stroked with blunt object (key) till the ball of little toe comes, then it is turned medially over the heads of metatarsals.
Motor system Response:
- Flexion of great toe at metatarsophalangeal joint.
- Other toe gets flexed.
- Ankle is plantar flexed and inverted
- Flexion of the knee and hip joint
- Contraction of adductors of the thigh, sartorius and tensor fascia lat
Motor system Extensor plantar response:
- Dorsiflexion of great toe (first occurs)
- Fanning out (spreading) of other four toes and extension of toes
- This response is pathognomonic of UMN lesion (pyramidal tract)
Motor system Other conditions causing Babinski’s response:
- Physiological response is infants (as pyramidal tract not yet developed)
- After an epileptic convulsion
- During deep sleep
- Intoxications (alcohol, metabolic encephalopathy).
Motor system Other methods of eliciting plantar reflex:
- Oppenheim’s sign – Pressing along the inner border of tibia
- Schaefer’s reflex – by pinching the Achilles tendon
- Chaddock reflex – by striking around the lateral malleolus
- Gonda’s reflex – by pressing one of the toes and releasing it suddenly.
- Gordon’s – by squeezing the calf muscle.
- Root value – L5 S1
- → In UMN lesions – extensor plantar response seen
- In LMN lesions – Plantar reflex absent.
9. Bulbo cavernous reflex – Pinching dorsum of glans penis.
- It leads to contraction of bulbo cavernous muscle.
- Root value – S3 S4.
Motor system Sphincteric reflexes:
- Swallowing any difficulty in swallowing
- Defecation – any incontinence (or) difficulty in defecation.
- Micturition – any incontinence.
Motor system Deep tendon reflexes in various lesions:
1. Inversion of supinators reflex – In lesions of C5 there is no contraction of brachio radialis, but there is flexion of middle and index fingers.
- Biceps reflex absent, but triceps is exaggerated.
- Brisk supinators reflex – flexion of fingers seen, but there is contraction of brachio radialis muscle.
2. Delayed relaxation reflex response – Hypothyroidism
3. Clonus – Increased reflex response.
- Ankle clonus – knee is flexed, ankle is dorsiflexed with a pressure suddenly. Sustained clonus – when the pressure released, still the clonus seen.
- Patellar clonus – Knee is extended, patella pushed downwarYou can seethe rhythmic contraction of the quadriceps muscle.
Motor system Co-ordination of movements:
- Upper limb finger-nose test – with eyes open, finger taken from lateral side and the tip of nose touched.
- This is also performed with eyes closed.
- With eyes open → if there is any past pointing represents cerebellar lesion.
- With eyes closed – he cannot perform this act and then there is sensory ataxia (lesions of posterior columns).
Motor system Lower limb:
- Knee – heel test – Heel of one leg touched the knee of other leg.
- Rest of the things are same as the above mentioned.
- Romberg sign – To test the loss of position sense (Sensory ataxia) (eyes closed)
- Patient is asked to stand with legs together (may be on toes) then he sways to the side of lesion.
- It is not usually performed for cerebellar ataxia.
Motor system Gait – It represents the stance:
Gait Types:
- Hemiplegi gait – circumduction – The affected leg is first thrown outside and then brought close to the opposite leg the affected arm is flexed.
- Reeling gait – Cerebellar lesions, gait is like a drunken person (zig-zag).
- Stamping gait – In sensory ataxia, patient stamps the ground as he does not feel the sensation of ground.
- High stepping gait – It is seen in foot drop (lesion of deep peroneal nerve) foot is raised high to overcome the foot droop.
- Festinant gait – seen in parkinsonism.
- Person takes small steps, he is leaning forward as though trying to catch his own center of gravity, he cannot control the speed – when pushed forward → he goes rapidly forward when pushed backward – he goes backward rapidly. He cannot properly change the direction.
- Walding gait – In paralysis of abductors of thigh (Gluteus medius, minimus).
- Fracture femur neck; Dislocation of Hip.
- There is swaying to the side of paralysis.
- When the paralysis seen on both sides – then, he sways towards both sides – lurching gait.
Gait Involuntary movements:
- Athetosis Writhing type of movements seen in distal than proximal group of muscles.
- Lesion in globus pallidus (basal ganglia).
- Hemiballismus – flailing type of movements of limbs (Ballistic flinging movements) seen in lesions of sub thalamic nucleus.
- Chorea – dancing type of movements (flickering) commonly affects distal muscles.
- Lesion seen in caudate nucleus.
- Tremors:
- Involuntary tremors – It is seen in parkinsonism. Tremor seen even at rest.
- Rotary component between finger and thumb (Pill-rolling tremor).
- Rapid rhythmic alternating tremor, predominantly in flexion (or) extension.
- Intention tremor – In cerebellar lesions, tremor starts when the person starts doing some work.
- Not seen at rest.
- Tremors also seen in thyrotoxicosis
- Flapping tremor (asterixis) – Hepatic encephalopathy, renal failure, cardiac failure, respiratory failure.
Gait Other involuntary movements:
- Myoclonus
- Dystonia
- Dyskinesia
- Myokymia – Twitchy movements of periorbital muscles
- Tetany – due to hypolakemia.
- Fasciculations – Rapid, irregular and inconstant visible twitching movements of muscle fibres.
4. Sensory system:
Sensory system Superficial senses:
- Touch- With a cotton wisp, touched to know the sensation of touch.
- It is mediated by posterior columns.
- Pain – A sharp pin with blunt head used to elicit pain. It is mediated by antero lateral system (lateral spinothalamic tract) superficial pain carried by as fibres
- Deep pain-‘C’ fibres.
- Temperature – Hot water, cold water placed in test tubes to test this sensation.
- This is mediated by lateral spinothalamic tract.
Sensory system Deep sensations:
- Vibratory sense- using tuning fork of 128 Hz, it is tested
- Tuning fork is struck and the vibrating tuning fork kept over the bony prominences – olecranon, mastoid, forehead etit is mediated by posterior columns.
- Position sense – Tested at the small joints – IP joints. Joint is kept stabilized by holding it, asked the patient to tell (eyes closed) to which side it is bent. It is tested in upper limbs, lower limbs.
- Pressure – Tested and carried by ventral spinothalamic tract.
Sensory system Cortical sensations:
- Requires integrity of sensory cortex.
- Tactile localization
- Tactile discrimination – Two point discrimination. Using two-point divider, it is testePatient is asked when he feels two different points (or) not.
- Fingers are most sensitive (Resolving 1-5 mm separation)
- Back, dorsum of foot least sensitive – 5 cm required.
- Stereognosis
- Recognition of shape, size, form of an object.
- Patient is asked to close his eyes, an object given to him and asked to describe the above parameters → it represents lesion in sensory cortex (posterior parietal area) provided there is no hypoaesthesia (or) anaesthesia of hand.
5. Autonomic function:
- It may be sympathetic – thoraco lumbar outflow
- Parasympathetic – cranio sacral outflow.
- Look-any:
- Postural hypotension
- Impaired sweating
- Urinary incontinence
- Urge incontinence – UMN lesion
- Overflow incontinence – LMN lesion
- Constipation
- GI dysmobility
- Impotence
- Erection failure.
6. Signs of meningeal irritation (meningiom):
- Neck rigidity – usually, chin touches the chest, when neck flexed, but without pain.
- In meningeal irritation, pain is felt.
- Kernig’s sign – Patient is in supine position. Hip is fully flexed then the knee is extendeThis causes pain in meningeal irritation.
- Brudzinski’s sign – knee is flexed, when the neck is passively flexeStraight leg raising test- usually performed for sciatica.
- When the extended leg is flexed at the hip, nerve sheaths are stretched leading to pain.
Signs of meningeal irritation (meningiom) Pathways:
1. Pyramidal Tract:
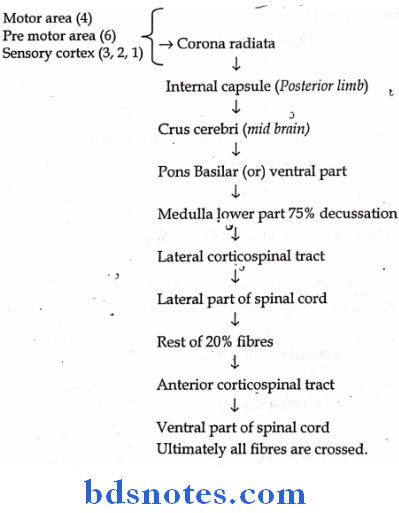
2. Difference between UMN lesion and LMN lesion
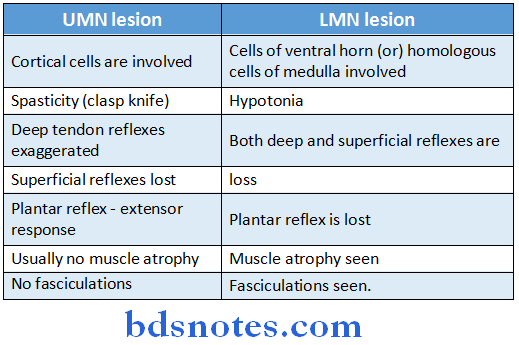
3. Dorsal columns (posterior columns):
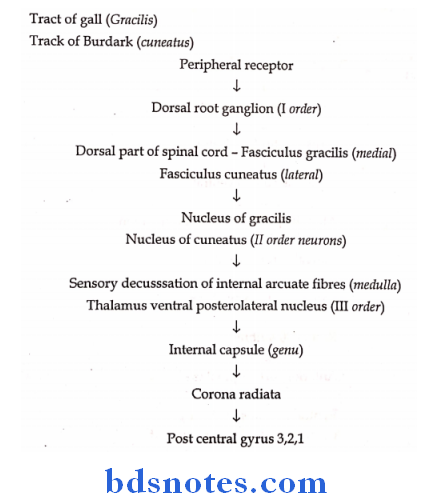
4. Anterolateral system:
- Lateral spinothalamic tract
- Ventral spinothalamic tract.
- Lateral spinothalamic tract- crossed – carries pain, temperature

Cases
Cerebro Vascular Accident:
Hemiplegia:
Name: Ramaiah
Age: 60 years
Sex: male
Address: East marredpally (Addagutta)
Occupation: Farmer
DOA: 15-01-2002
Chief complaints : not able to move left upper and lower limbs.
H/o patient illness : Patient apparently asymptomatic 4 days bacHe developed pain in the neck muscles on 15th morninHe applied amruthanjam and slept for sometimAs soon as he woke up, he fell down while trying to walk and found that his left upper and lower limbs were paralysed (not able to move).
Paralysis is sudden in onset and involved whole of the limbs.
Hemiplegia Non progressive 4 days duration:
- No H/o Fever
- No H/o Chest pain
- No H/o Breathlessness
- No H/o Palpitation
- No H/o Syncopal attack No H/o Convulsions
- No H/o Trauma (Head injury)
- No H/o Dysarthria
- No H/o Urinary incontinence
- No H/o Headache; vomiting
- No H/o Loss of consciousness
- Mouth deviated slightly to right side.
- No accumulation of food in between teeth and check.
1. Motor – Proximal – ask for combing hair getting up from chair
- Distal – eating able to hold the slippers
2. Sensory – Any tingling sensations wash basin attack
3. Cranial
- III – PTOSIS, Diplopia
- IV, VI- Diplopia
- VII – deviation of mouth
4. Autonomic
- Symptoms – H/o postural hypotension
- Increase or decrease sweating etc,
- Cough – Since 1 year, productive, thick, mucoid associated with breathlessness.
Hemiplegia Past history:
- No diabetes, tuberculosis and asthmIt is hypertensive but not known RHD, IHD, TIA.
Hemiplegia Family history:
- No similar complaints seen in the family members. No H/o IHD, DM.
Hemiplegia Personal history:
Diet: mixed
Appetite : normal
Sleep: normal
Addiction: Smoking since 45 years
3-4 beedis/day
Not an alcoholic.
Hemiplegia Drug history:
- He has not taken medicines, not significant.
Hemiplegia General examination:
- Patient is average built and moderately nourished; conscious, coherent and comfortable in lying down position
- upper limb→ flexed; lower limb – extended
- Skull, spine – normal.
- No neurocutaneous markers.
Hemiplegia Vital data:
- P-x
- I-x
- C-mild
- K-x
- L-x
- E-mild.
Hemiplegia Vital signs:
- Temperature – Normal
- Pulse rate-60/min
- Rhythm – not regular character – volume; condition of vessel wal
- BP-180/90
- Respiratory rate – 20/min, regular, abdomino thoracic.
Hemiplegia Systemic Examination:
- Intellectual functions:
- Consciousness: He is conscious and answering questions
- Behaviour: no abnormality noticed
- Emotional stale: he is calm
- Orientation (place and time): answered questions where is he now?
What may be the time? - Memory: able to tell the meal taken by him last night.
- Intelligence: answered simple calculations.
- Speech and language: No dysarrthria, No aphasia able to understand, listen what we asked.
Hemiplegia Cranial nerves right/left:
I-nerve : Feel smell
II- nerve : Visual acuity visual field
III- nerve: Occular movements
IV- nerve:Occular movements
V-nerve: Trigeminal – feeling sensations over face
VI- nerve: Occular movements
VII-nerve : Mouth in slightly deviated towards right side
VIII- nerve: Not deaf
IX- nerve :Palatal reflex, taste sense over post 1/3 tongue
X- nerve : Uvula in normal position, palatal reflex normal
XI- nerve Shrug his shoulders and also sternomastoid
XII- nerve: Normal (Hypoglossal) – No deviation of tongue noticed after protrusion.
Hemiplegia Motor system:
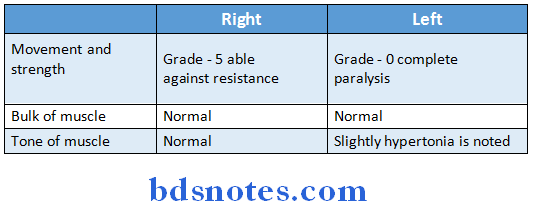
Hemiplegia Reflexes:
- Tendon reflexes grade – Knee, ankle, biceps, supinators, triceps – exaggerate
- Superficial reflexes – plantar reflex, extensor plantar response.
- Babinski’s sign +ve dorsiflexion of foot with fanning of finger extension of great toe.
- Abdominal reflex – not elicited
- Corneal reflex
- Sphincteric reflexes:
- Swallowing
- No urinary incontinence
- Defaecation constipated for last 3 days.
Hemiplegia Autonomic function:
- No urinary incontinence
- Sweating normal
- No postural hypotension (no syncope when in erect posture)
Hemiplegia Diagnosis:
- Upper motor neuron lesion → spastic paralysis
- Babinski’s sign +ve
- Thrombosis of MCA as there is no headache, Vomiting, convulsions; CVS is within normal limits. (Mainly internal capsule)
- Left Hemiplegia.
Patient illness:
1. Motor system:
- Proximal
- Myopathies
- Upper limb – combing hair
- Lower limb getting up from sitting, climbing stairs
- Myopathies
- Distal
- Corticospinal lesions
- Upper limb – buttoning short.
- Lower limb – wearing slippers
- Corticospinal lesions
2. V and XII nerves – deviated to paralysed side VII and X nerves – deviated to normal side
3. Autonomic – sweating (impaired), urinary incontinence, constipation, impotence, postural hypotension.
- CVS complaints – palpitation, chest pain, bradycardia.
- OC pills in case of females (may cause thrombo umbolism)
- Past history – Previous hemiplegic attack (transient ischemic attack TIA -for 24 hr). RIND (Reversible ischemic neuronal deficit) – for 1 week.
Neuro cutaneous marker – Café and lait sports (Neurofibromatosis) right
- Hypopigmentation (Hansen’s)
- Thickened nerves
- Haemangiomas.
4. Cortical lesion – unconscious seizures may present. Internal capsule – conscious no seizures.
Patient illness Discussion:
1. What is the lesion
- The lesion is CVA can be thrombosis, embolism (or) haemorrhage.
Patient illness Cerebral thrombosis:
- The patient may be hypertensive and atherosclerosis present.
- It is not that much rapid as that of embolism.
- Past history of TIA may be present.
- It may occur during sleep (or) soon after getting up from be
- There is no migration of hemiplegic site.
Patient illness Embolism:
- Underlying heart disease may be present (valvular heart disease atrial fibrillation)
- Attack develops rapidly (within seconds)
- Headache, convulsions are usually not seen.
- Past history of TIA may not be seen.
- There is migration of hemiplegic site.
Patient illness Intracerebral haemorrhage:
- Person usually hypertensive
- Attack occurs during exertion
- Headache, vomiting (↑ ICT) convulsions may be present.
- Features of atherosclerosis may be present.
- Most common site of hypertensive bleed → putamen then, thalamus.
2. Where is the lesions:
Lesion may be cortical, sub-cortical, internal capsule, brain stem, spinal cord.
Cortical lesion:
- Cortical lesions are usually associated with loss of consciousness sand seizures.
- Usually monoplegia is seen. (As fibres are distributed widely, to produce hemiplegia extensive area to be involved).
- Cortical sensory loss present
- Lost
- Asterognosis.
- Tactile discrimination
- Lost
3. Jacksonian convulsions can occur.
Sub cortical (Corona radiata):
- Similar to cortical lesion, monoplegia is common, but hemiplegia is more common than that of cortical lesions.
- Loss of tactile discrimination may he seen due to involvement of thalamo cortical fibres.
- Conscious.
Sub cortical (Corona radiata) Internal capsule:
- It is the most common site, usually involved.
- So many fibres are clustered in a small plac
- So even a small lesion can produce hemiplegia.
- On involved side
- Upper limb – flexed
- Lower limb-extended
- Hemianaesthesia, homonymous hemianopia occurs.
- UMN type of facial N. palsy (supra nuclear palsy).
Sub cortical (Corona radiata) Brain stem:
- Crossed hemiplegia – facial palsy seen on one side and the hemiplegia seen on other side.
- Associated cranial nerve involvement on the side of lesion and opposite hemiplegia.
- Associated gaze paralysis (center is PPRF parapontine reticular formation).
- Change in pupil size (dilated in III N. lesions constricted in pontine haemorrhage).
- Mid brain – III, IV;
- Pons – V, VI, VII, VIII
- Medulla IX, X, XI, XII
Brain stem involving disorders:
- Weber’s syndrome – lesion in anterior cerebral peduncle (mid brain)
- Ipsilateral 3rd nerve palsy
- Contra lateral upper motor neuron 7th nerve palsy
- Contra lateral hemiplegia.
- Millard gubler syndrome – lesion in ponto – medullary junction
- Ipsilateral 6th nerve palsy
- Ipsilateral UMN VII nerve palsy
- Contralateral hemiplegia.
- Wallenberg syndrome (lateral Medullary syndrome)
- Due to thrombosis of PICA (posterior inferior cerebellar artery) Involving lateral medulla.
- Medial medullary syndrome – XII nerve invoted (opposite site)
- Ipsilateral V, IX, X, XI N. palsy
- Ipsilateral Horner syndrome
- Ipsilateral cerebellar signs
- Contralateral spinothalamic (pain, temp loss pressure).
- Vestibular disturbance.
- Spinal cord – usually quadriplegia, paraplegia associated LMN signs present.
3. Causes of limb weakness:
- Vascular lesions – as described above- thrombosis, embolism, bleed usually sudden onset (over minutes) followed by stable period and gradual recovery.
- Inflammatory causes – multiple sclerosis
- Acute onset (over days)
- Persist for sometime and then the condition improves.
- Neoplastic conditions
- Gradual and progressive over weeks (or) months
- Associated signs of raised ICT → Headache
- Vomiting
- Convulsions.
- Degenerative conditions:
- May be taken over months (or) years.
- Example: Motor neuron disease
- Cervical spondylotic myelopathy.
4. Manifestations due to involvement of various territories
Anterior cerebral artery involvement (ACA):
- When ACA involves distal to the anterior communicating artery causes weakness, cortical sensory loss more of contralateral leg than hand, grasp reflex, parotonic rigidity, lack of initiative, urinary incontinence present.
- When ACA involved proximal to ant. Communicating artery, it is better tolerated due to extensive collaterals.
Middle cerebral artery (MCA):
- Hemiplegia, hemi sensory loss, Homonymous hemianopia, eyes are deviated to the side of lesion.
- If dominant hemisphere involved – aphasia seen
- Non-dominant- apraxia; anosognonia (Negligence of paralysed limbs).
- Apraxia – Not able to do certain acts even though no sensory (or) Motor disturbances noted.
- Example: When match box given to him and explained him what to do but not able to know how to use the matchbox.
Posterior cerebral artery (PCA):
- Leads to thalamic syndrome – contralateral hemisensory loss, spontaneous pain, hyperpathia.
- Macular sparing homonymous hemianopia
- A temporary hemiparesis.
Verterbro basilar system:
- Vertigo, ataxia, diplopia, dysarthria, blurring of vision, perioral numbness, paraesthesiias and weakness (or) sensory complaints on one (or) both (or) alternating sides of body.
Internal carotid artery:
- Dysphasia, mono occular visual loss (due to amaurosis figax) in the eye contra lateral to the affected limbs.
- Hyper reflexia, extensor plantar response
- Presence of carotid bruit, cardiac abnormality
- On examination, usually no neurological abnormality found.
5. Risk factors for CVA:
- Valvular heart disease, atrial fibrillation
- Diabetes mellitus
- Systemic hypertension
- Atherosclerosis (Hyperlipidemias)
- Obesity
- Smoking, alcohol consumption
- Oral contraceptive pills in females
- Hyperviscosity → Polycythemia; bleeding conditions – thrombocytopenia
- Trauma.
6. Causes for stroke in young:
- Underlying cardiac disease causing embolism
- Familial conditions (Hyperlipidemia, diabetes, hypertension)
- Multiple sclerosis (demyelination)
- Arteritis (as a result of syphilis, Takayasu arteritis)
- Hyperviscosity – Thrombocythaemia, polycythemia
- Bleeding diathesis – Leukaemia, thrombocytopenias (ITP)
- Tuberculoma, cerebral malaria
- Lateral sinus thrombophlebitis puerperium
- Encephalitis, intracranial neoplasms
- Anti phospholipid syndromes – LA, ACAS
7. Causes of recurrent hemiplegia:
- Transient ischaemic attacks (usually embolism)
- Multiple sclerosis
- Hemiplegic migraine
- Hypertensive encephalopathy
- Todd’s palsy – post epileptic palsy.
8. Investigations for CVA:
- Routine – CBP, ESR, RBS, Blood urea, X-ray chest.
- Specific
- Lipid profile (LDL, HDL, TG)
- ECG to know any cardiac disease
- 2D echocardiography – to know any cardiac disease
- Doppler study of carotids (any carotid stenosis) to know valvular heart disease.
- CT scan – Opacity seen (bleed)
- Transluscency (Infarction)
- Any space occupying lesion.
- Carotid angiography
- General Medicine
- Lumbar puncture – xerochromia seen incase of subarachnoid haemorrhag
- Screen for LA (Lupus anticoagulant)
- ACA (anti cardiotipin antibody)
- Homocystein levels (homocysteihemia causes thrombosis).
9. Management
- Cerebral infarction:
- Supportive:
- Ryle’s tube insertion, Ryle’s tube feeding.
- Foley’s catheter placed in case of incontinence.
- Good nutrition to the patient.
- Good nursing care so as to prevent bed sores, infections.
- Broad spectrum antibiotics used.
Management Specific:
- CT scan is donIf thrombosis confirmed then only treatment started.
Management Thrombolytic therapy:
- Usually right PA (recombinant tissue plasminogen activator) is helpful when given within 3 hours.
- 0.9 mg/kg maximum 90 mg
- (10% of the drug given as bolus, rest given in an hour)
Management In acute stage, to relieve cerebral edema.
- By dexamethasone
- Dehydrating hyperosmolar gents – mannitol, glycerol given.
- Anti platelet drugs – Aspirin
- Clopidogrel, ticlopidine
- Abciximab (IIb/IIIa receptor antagonists)
- Anti coagulants (oral) – in case of underlying cardiac disease they are given Warfarin given with INR maintained at 2-3
- Physiotherapy – It is important.
Cerebral haemorrhage:
Supportive care as mentioned above:
Specific:
- Hyperosmolar agents – 20/mannitol, oral glycerol in lime juice
- InDexamethasone – 4-6 mg IV 6 hrly
- Antihypertensives control B.P.
- Anti lipideic drugs
- Physiotherapy.
Alimentary System
Case Proforma:
Name :
Age:
Sex : Primary biliary cirrhosis common in females
Address:
Occupation
Date of admission:
Chief complaints:H/o present illness.
Appetite
Loss of appetite:Gastric carcinoma
:Hepato cellular damage
:Anorexia nervosa – seen in young females
Excessive appetite :Parasitic infections
:Psychological
:Diabetes mellitus
:Hyperthyroidism.
Vomiting:
1. What is the duration
2. Is it progressing
3. Quantity
- Large quantity in pyloric obstruction
- Small quantity – esophagitis, gastritis.
4. Odour
- Peculiar acid smell (sour) represents
- Pyloric obstruction
- When this is absent – due to achalacia cardia zenker’s
- Diverticulum Faecal odour – Intestinal obstruction
5. Colour:
- Gastro colic fistula.
- Coffee ground – dark brown coloured vomiting.
- It is due to formation of acid hematin (usually gastric origin)
- Greenish – Bile present in vomiting
- Bilious vomiting – Pyloric obstruction
- Non bilious vomiting – Small intestine obstruction
- Esophageal (achalacia; zenker’s).
6. Contents of vomiting:
- Normally mucus, partially digested food present
- Excessive mucus represents gastric carcinoma prolonged stasis of food in stomach.
- Food vomited which was eaten 8 hr ago – pyloric obstruction
- Repeated vomiting of food – achalacia cardia.
7. Whether it is projectile (or) non projectile
Projectile vomiting represents – autonomic disturbance.
8. Timing-Early morning vomiting
- Pregnancy
- CRF
- Alcoholic gastritis
- Raised intracranial tension.
Vomiting that occurs 2-4 hr after food – gastric ulcer.
Alimentary System Hemetemesis:
Blood vomiting (It usually represents bleeding above duodenal sphincter).
1. How is the onset
2. Duration, progression
3. Quantity of blood vomited (to assess severity, for blood transfusion)
4. Red colour due to vomiting immediately after bleeding
- Dark red (or) brown vomiting after sometime (acid hematin formed).
- Ask for – abdominal pain relieved by food (Duodenal ulcer) (or) aggravated by food (gastric ulcer).
- Any H/o alcoholic intake (alcoholic gastritits)
- Any H/o NSAID abuse
- Any H/o Hepatocellular damage (esophageal varices).
Alimentary System Abdominal pain:
1. Sudden onset (or) gradual onset
2. Duration, Progression
3. Site of pain:
- Right hypochondrium
- Cholycystitis
- Hepatitis
- Pleurisy
- Lower pneumonia
- Right iliac fossa
- Appendicitis
- Renal colic
- Pain in epigastrium – gastric origin (gastritis)
4. Character of pain – Pricking, Stabbing, Colicky (due to intestinal obstruction).
5. Timing any diurnal variations (more during day (or) night) person gets up with abdominal pain – Duodenal ulcer.
- Timing with food-Pain relieved by taking food – duodenal ulcer
- Pain aggravated on taking food – gastric ulcer.
6. Any radiation of pain:
- Pain in epigastrium radiating to back – pancreatitis
- Pain in right hypochondrium radiating to shoulder- cholycystitis (inter scapular space)
- Pain felt around epigastrium – from foregut
- Around umbilicus – from mid gut structures
- Around hypogastrium – hind gut origin.
- Pain from groin to loin – ureteric colic.
- Pain around umbilicus, gradually radiating to right iliac fossa – appendicitis.
- Ask for any associated vomiting (Intestinal obstruction).
Alimentary System Abdominal distension:
1. How is the Onset (gradual distension – ascites)
2. Duration, Progression
3. Distension-localized (or) generalised
- Ask for
- Hepatic cause for ascites
- any H/o vomiting
- H/o jaundice
- Hepatic cause for ascites
- H/o chest pain
- H/o dyspnoea → Ascites can also cause dyspnoea by diaphragm elevation.
- CVS cause
- H/o palpitations
- H/o pedal edema
- H/o oliguria, anuria
- CVS cause
- Renal cause
- H/o hiccups
- H/o facial puffiness
- H/o altered bowel habits
- H/o associated abdominal pain (spontaneous bacterial peritonitis)
- Koch’s disease
- H/o cough
- H/o evening raise of temperature
- H/o night sweats
- In females ask for menstrual history
- Any irregularity (Menorrhagia Polymenorrhea Post coital bleeding).
- Ovarian Ccan cause ascites.
Alimentary System Hiccups (Singultus):
- Due to irritation (or) Contraction of diaphragm.
Hiccups (Singultus) Causes:
- Phrenic neuritis
- Uremia
- Cirrhosis of liver
- Cardiac failure.
- Space occupying lesions of brain
- Meningitis (or) encephalitis
- Following abdominal surgery
- Diaphragmatic hernia
- Pericarditis.
Hiccups (Singultus) Loose motions:
1. Onset, Progression, Duration → Acute (or) chronic
- Chronic diarrhoea (>14 days)
2. No. of episodes (frequency)
3. Any associated blood and mucus – dysentery
- Associated pus – infection
4. Quantity
- Large quantity
- Amoebic dysentery
- Giardiasis
- Steatorrhea
- Small quantity
5. Colour – Dark (or) black tarry → (malena) – upper GI bleed
- Pale coloured – steatorrhea
6. Consistency-Solid, semi solid, watery
- Rice water stools – cholera.
7. Any associated tenesmus – bacillary dysentery.
Difference between Hemetemesis, Hemoptysis
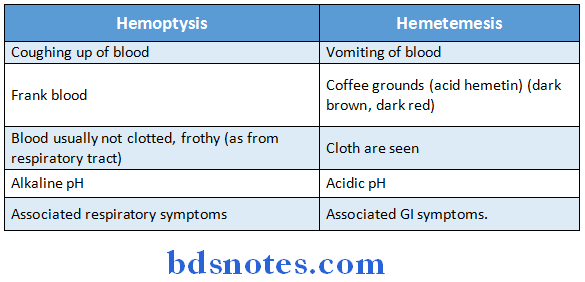
Jaundice (yellowish discoloration of sclera):
1. Onset – Rapid (or) Insidious
2. Duration – to assess severity
3. Progressing (or) not
- Ask for H/o fever
- Nausea, vomitng
- Hemetemesis
- H/o yellow discoloration of urine Infective hepatitis
- Nausea, vomitng
- H/o yellow discoloration of urine pruritus
- Ho pale coloured stools
- Cholestatic jaundice due to obstructive pathology
- H/o associated colicky abdominal pain – Biliary colic.
- Hepatitis B, Hepatitis C
- H/o previous blood transfusions H/o exposure
- H/o loss of appetite
- Malignancy (Hepatoma, Cholangio, Carcinoma)
- H/o significant loss of weight
- H/o Alcoholism
- H/o drug intake:
- Tetracycline (fatty change).
- Paracetamol (hepato toxic)
- Chlorpromazine (cholestasis)
- Methotrexate (fatty change)
Jaundice (yellowish discoloration of sclera) Ask for negative history:
- H/o irregular menses
- H/o anorexia, nausea, vomiting
- H/o yellowish discoloration of sclera
- H/o fever
- Hepatic failure
- H/o loss of hair
- H/o loss of libido
- H/o confusion
- Hepatic failure
Ask for negative history Past history:
- Any similar complaints in the past.
- Any past H/o TB, Jaundice, Rheumatic heart disease.
- Any known H/o diabetic/HTN.
Ask for negative history Family history:
- Any similar complaints in the family
- Any H/o contact with TB
- Can be heritable
- Hemochromatosis
- Wilson’s disease
- α, AT deficiency
Ask for negative history Menstrual history:
- In females it is important to ask for
- H/o irregularity of cycle
- H/o ↑ bleeding
- H/o ↑ duration (ask no. of days of bleeding) H/o post coital bleed
- H/o pain during menstruation.
Ask for negative history Personal history:
- Appetite
- Sleep
- General Medicine
- Micturition
- Bowel movements
- Addiction – any smoking, alcoholism
Ask for negative history Drug history:
- Any H/o intake paracetamol
- Methotrexate
- Tetracycline
- Chlorpromazine
- Chloroquine
Ask for negative history General examination:
- Built/Nutrition
- Patient conscious/coherent/comfortable
- Top-loe examination → it is important
- Look for hepatic failure signs and other related – any pigmentation (hemo chromatosis)
- K-F ring (Wilson’s disease).
- Hepatic failure – palmar erythema
- Spider naevi
- Arterixis (hepatic encephalopathy)
- Endocrinal- loss of hair
- Loss of libido
- Retor hepaticus (due to mercaptans)
- Dupytron’s contracture (flexion of ring finger)
- Meralgia paraesthesia (entrapment of lat cut N. of the thigh)
- Any parotid swelling.
Ask for negative history Measurements:
1. Transverse abdominal girth at umbilicus
2. From xiphisternum to umbilicus
3. From umbilicus to pubic symphysis
4. Spino umbilical distance
- Equal in both sides in Axites
- Symmetrical in ovarian cyst.
Ask for negative history Vital signs:
Pickle:
- Pallor, icterin, cyanosis, Koilonychia, lymphadenopathy, edema – described under spotters.
Ask for negative history Vital data:
- Temperature
- Pulse rate
- BP
- Respiratory rate.
Ask for negative history Systemic examination:
- Examine
- Oral cavity
- Lips
- Teeth
- Gingiva
- Tongue
- Buccal mu cos a
- Abdomen (or) Inspection
- Shape of abdomen
- Normally scaphoid in thin individuals
- Flat abdomen in young
- Protruded due to accumulation food.
- Usually umbilicus central in position
- When flanks are more distended ascites
- Shape of abdomen
- Distended abdomen can be due to – Fat
- Fluid (ascites)
- Flatus
- Faeces
- Full bladder
- Fata (Any growth)
- Ascites generalised abdominal distension.
- Localized abdominal distension
- In hepatomegaly
- Splenomegaly
- Any growth
- Localized abdominal distension
2. Umbilicus
- Normal umbilicus – central and inverted
- Transverse (or) Smiling umbilicus -Ascites
- Vertical drawn up – ovarian cyst
- Everted umbilical hernia
- Bluish discoloration of umbilicus – Cullen’s sign (pancreatitis ruptured ectopic pregnancy).
- Any metastatic nodules to umbilicus – Sister Joseph’s nodules (from gastric carcinoma)
- Red umbilicus-inflamed Meckel’s Diverticulum.
3. Skin over abdomen – Whether it is
- Ascites; pregnancy
- Shiny
- Stretched
- Linea albicantes striae
Look sinus, scars, dilated veins (caput medusac, flank veins).
4. Movements of abdominal wall
- Whether all quadrants equally moving with respiration (or) not
- Complete absence of movements → peritonitis
- In ascites, may be reduced
- 1,3 Hypochondrium (right, left)
- 2 Epigastrium
- 4,6 Lumbar regions
- 5 Umbilical region
- 7,9 Iliac fossa
- 8 Hypogastrium.
5. Divarication of recti – examine the rectus muscles
- If there is wide gap between the two (Divarication potential danger for epigastric hernia).
6. Visible peristalsis
- From left to right going horizontally – pyloric stenosis
- When the person asked to take some water it can be easily demonstrated.
7. Hernial sites – Don’t forget to examine
- Ascites may cause hernia
- Femoral hernia
- Inguinal hernia – Inguinal canal (medial is above inguinal ligament)
- Umbilical hernia
- Vertical hernia (Incisional Hernia).
8. External genitalia
External genitalia Palpation:
1. Temperature – Raised (or) not
2. Tenderness – Present (or) not
Rebound tenderness – peritonitis
Doughy abdomen – TB.
3. Guarding – It is due to muscular contraction. It can be voluntarily relaxe
4. Rigidity – Muscular contraction over inflamed region.
- It cannot be relaxed voluntarily.
- Seen in Peritonitis
- Perforation of visus
- Acute pancreatitis, cholecystitis
- Intestinal strangulation
- Seen in Peritonitis
5. Harvy sign – To detect the direction of blood flow in dilated veins.
- A straight veins selected.
- By using two index fingers of both hands, vein is emptied.
- The above finger released – if blood flows from above – down – obstruction of SVC.
- Lower finger removed → If blood flows below upwards → obstruction of IVC.
6. Viscera
- Before palpation, legs are flexed and examines should stand on right sidHands are walmed.
- If legs are not flexed – Ilio tibial tract is stretched, which also stretches abdominal wall muscles there by interfering with examination.
- Liver – It is palpated by right hand, starting from right iliac fossa gradually upwards towards right hypochondrium.
- If liver is palpable→ say as how many finger breath below costal margin.
- Liver moves with respiration
- Palpate inferior border – smooth (or) sharp
- Surface regular, smooth (or) not look for any tenderness.
- When liver is palpable (Hook method)→ fingers cannot be insinuated below margin.
Spleen – with right hand, right iliac for a palpated, then gradually upwards, obliquely towards left hypochondrium
- Classical method
- Hooking – if splenomegaly present, fingers can not be hooked below costal margin.
- When spleen palpable – say how many cm (or) finger below costal margin
- It moves with respiration
- Spleenic notch is palpable.
- Dipping method – When severe ascites present, this method usefu
- It is similar to classical method except that the examiner dipping the fingers every time he palpate.
- Kidney (Left kidney)
- Bimanual palpation – stand on right side of patient. Place the right hand in the left lumbar region, left hand placed posteriorly in the loin; patient asked to take breathing, left hand pressed, kidney palpable in between two hands.
- It can pushed from one hand to another (Ballotable)
- It does not move with respiration.
- Similarly right kidney palpable.
- Gall bladder – method is similar to liver palpation.
- When gall bladder enlarged – smooth globular swelling with distinct borders felt below the inferior border of liver.
- Bladder – full bladder can be palpable.
- Aorta, common vessels palpated for any aneurysms.
- Extend genitalia – Don’t forget to palpate the external genitalia.
External genitalia Percussion
1. Shifting dull ness:
- In moderate ascites (750-1000 ml)
- Left middle finger (Pleximeter)
- Right middle finger (Plexor)
- Percussion started from the xiphisternum in midline, gradually downwards upto umbilicus then laterally towards flanks until dull note hearWhen dull note is heard, left finger placed on that point and the patient is asked to turn laterally to the opposite sidWait for 1-2 mm till the fluid shifts more anteriorly, then percuss, it gives resonant notAgain patient asked to turn straight. After sometime when percussed it again gives dull note.
2. Fluid thrill:
- In massive ascites
- Patient is asked to place his hand vertically over center of abdomen. In order to prevent abdominal wall vibrations to other side.
- You place your left hand in the opposite flank, with right hand give a flick, fluid thrill felt over the left hand.
3. Puddle sign – Minimal ascites (150 ml):
- Patient is asked to be in knee-heel position, so that fluid gets accumulated more anteriorly.
- On one of the flanks, a click given, and the most dependent part is auscultated with stethoscope (fluid movement heard).
- When auscultated on the opposite flank no fluid movement heard.
4. Percussion of viscera:
- Liver Start percussing from 5th ICS over mid clavicular line on right side, gradually progress down even on to the abdominal wall till resonant note heard.
- Note the distance from 5th ICS→ to the point of resonance → it gives liver span (normal 12-15 cm).
- Spleen – spleen is usually not percussable.
- When enlarged → abdominal wall percussed from left costal margin over left hypochondrium.
- Measure the spleen size below costal margin.
- Urinary bladder – By percussion, full bladder can be detected
- Start percussing from below umbilicus – if dull note is heard, it is usually full bladder.
External genitalia Auscultation:
1. Peristalic movements
- Auscultate just to the right of umbilicus
- When absent – Peritonitis
- Paralytic Ileum.
2. Arterial bruit – renal artery – just above and left to umbilicus
- Bruit heard in renal artery stenosis.
- Bruit heart in right hypochondrium
- Tricuspid regurgitation
- Haemangioma of liver
- Hepatoma
3. Venous Hum
- (Curvilinear baumgarten syndrome)
- Umbilical collateral vessels give venous hum in cirrhosis.
External genitalia Other system examination
1. CVS:
- Hepatic manifestations seen
- Constrictive pericarditis
- Cardic failure
- Rheumatic heart disease
2. Respiratory system:
- Cor pulmonale
- Pleural effusion
3. CNS-Hepatic encephalopathy – Neurological signs present
4. Renal – Hepato renal syndrome can hamper – Kidney function.
External genitalia Diagnosis:
Diagnosis Ascites due to:
- Cirrhosis of liver
- Tuberculosis etiology.
Cases
Ascites:
Name:
Age:
Sex:
Address:
Occupation:
Chief complaints: Distension of abdomen.
Blood vomitings (hemetemesis)
Vomitings
Breathlessness
H/o present illness:
- Expand the chief complains as described in the previous section.
H/o present illness Vital signs:
H/o present illness Vital data:
H/o present illness Systemic examination:
Systemic examination Inspection:
- Distended abdomen, flanks are full.
- Skin is shiny, stretched, linea albicantes may be present.
- Divarication of recti may be present.
- Distended veins may be seen over the flanks Over the abdomen.
- Umbilicus is transverse, shifted downwards.
- Hernial sites are inspected for any hernia including external genitalia.
Systemic examination Palpation:
- Confirm the inspectory findings.
- Look for any rigidity, guarding.
- Any tenderness represents spontaneous bacterial peritonitis (or) Secondary infection.
- Determine the direction of flow in veins (Harvy’s sign).
- Palpate the viscera – use the dipping method.
- Take measurements of abdomen – In ascites length between xiphisternum and umbilicus is greater than that from umbilicus to pubic symphysis.
- Palpate external genitalia.
Systemic examination Percussion:
- Look for shifting dullness
- Fluid thrill (or)
- Puddle sign.
- Percuss the visceral organs to detect organomegaly.
Systemic examination Auscultation
- Look for bowel sounds
- Any other sounds – Arterial bruit
- Venous hum
Diagnosis – Ascites due to
- Tuberculous etiology
- Cirrhosis of liver.
Systemic examination Discussion:
- Etiology of Ascites
- Exudate
- Tuberculous
- Spontaneous bacterial peritonitis, other infections
- Pancreatitis
- Obstruction of thoracic duct
- Malignancy (lymphoma, leukaemia and other)
- Budd-chiari syndrome.
- Transudate
- Cirrhosis of liver
- Nephritic syndrome
- CCF
- Myxedema
- Protein losing enteropathy Meig’s syndrome
- Constrictive pericarditis.
Systemic examination Causes of chylous ascites
- White, milky peritoneal fluids due to presence of lymph.
- It contains lipid particles mainly triglycerides.
- Tuberculosis
- Obstruction to thoracic duct (or) Injury
- Filariasis
- Abdominal malignancy.
Systemic examination Haemorrhagic ascites (causes):
- Tuberculosis
- Traumatic conditions
- Malignancy
- Coagulation disorders
- Haemorrhagic pancreatitis.
Difference between Transudate and Exudate:
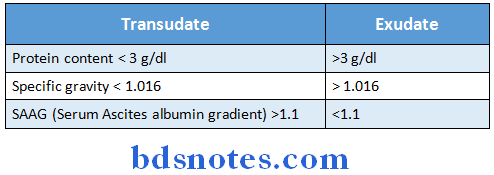
Difference between Ascites and Ovarian cyst:
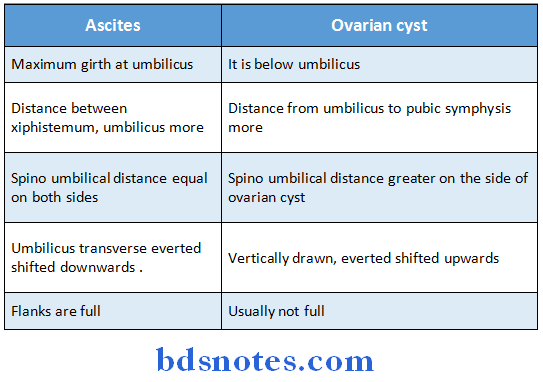
Systemic examination Investigations:
- Routine investigations
- CBP
- ESR
- RBS, Blood urea
- CVE – Proteinuria seen in nephritic syndrome.
- Specific
1. LFT to know the function of liver
- Serum proteins – hypoprotenemia seen in → Cirrhosis of liver
- Protein losing enteropathy Nephritic syndrome.
2. Lipid profile – Increased lipids in – Nephrotic syndrome
- Myxedema.
3. Ascitic fluid analysis – For gram stain/AFB stain
- Cell count
- Protein count
- SAAG (Serum Ascites albumin gradient)
4. X-ray abdomen – shows opacity
5. Ascites detected by USG abdomen (as little as 30 ml fluid)
6. For tuberculosis – Ascitic fluid – AFB stain
- Cell count – lymphocyte are increased Low albumin content
- SAAG <1.1 g/dl
Ascitic fluid – ADA (Adenine deamianase) levels
- PCR (Polymerase chain reaction)
- Bactec (for culture)
7. Portal hypertension – Doppler study of portal system to detect→ portal vein thrombosis.
8. Liver biopsy to confirm cirrhosis of liver.
9. Send
- HBs Ag
- HBc Ag
10. Serum electrolytes – hypokalemia, if present, leads to hepatic encephalopathy.
Systemic examination Management:
1. Bed rest-In lying down position, renal perfusion increases
- So increased diuresis leading to ↓ Ascites.
2. Salt restricted diet
3. Correct the electrolyte levels in serum
4. Diuretics Frusemide in combination with spiranolactone used.
5. Restriction of water intake.
6. Paracentesis – Ascitic fluid tapped at midpoint between spinoumbilical line and aspirate fluid.
- For every 1 litre of fluid aspiration 6 g salt free albumin is infused.
7. Leveen shunt – peritoneal fluid shunted into internal jugular vein.
8. TIPSS-trans jugular intra hepatic portal systemic stant.
A stent placed between intra hepatic portal system to IVC through jugular vein to decrease portal hypertension.
9. Distal leino renal shunt
- Splenic vein anastomosed to renal vein.
- It gives better results than TIPPS. Subsequent hepatic encephalopathy is less.
10. Treat the primary cause
- Tuberculosis – ATT
- Nephritic syndrome – steroids
- CCF Diuretics and vasodilators
- Myxedema – Thyroxin (T4) given Malignancy-remove the tumor.
Systemic examination Indications for abdominal paracentesis:
- Refractory to medical therapy
- Discomfort as a result of massive ascites
- Danger of strangulated umbilical hernia
- Diagnosis of etiology of ascites.
Systemic examination Portal hypertension
- Normal portal vein pressure 5-10 mm of Hg
- > 10 is usually portal hypertension.
- Triad – Splenomegaly
- Ascites
- Hemetemesis (due to variceal bleed)
Systemic examination Etiology of portal hypertension:
- Extrahepatic post sinusoidal – Budd chiari syndrome
- Intrahepatic post sinusoidal – veno occlusive disease Sinusoidal cirrhosis
- Intra hepatic pre sinusoidal – sehistosomiasis
- Extrahepatic pre sinusoidal – Portal vein thrombosis.
Systemic examination Complications of portal hypertension
Variceal bleeding
- Congestive gastropathy
- Hyperspleenosm
- Ascites
- Renal failure
- Hepato renal syndrome
- Hepato pulmonary syndrome
- Hepatic encephalopathy.
Systemic examination Factors precipitating hepatic encephalopath:y
- Constipation
- Hypokalemia
- Variceal bleeding
- Uremia
- Alkalosis
- Hyperventilation
- ↑ diuretic usage
- Sedatives, hypnotics, antidepressants
- Trauma
- Portal systemic shunts.
Systemic examination Clinical features of cirrhosis of liver:
- Jaundice
- Ascites
- Spider telegectasia, palmar erythema
- Cyanosis
- Endocrine loss libido, loss of hair
- Gynecomastia, testicular atrophy, impotence in men
- Breast atrophy, amenorrhea – in woman
- Epistaxis, menorrhagia
- Splenomegaly, fetal hepaticus
- Hepatic encephalopathy
- Pigmentation, clubbing.
Systemic examination Child-Pugh criteria for prognosis of cirrhosis
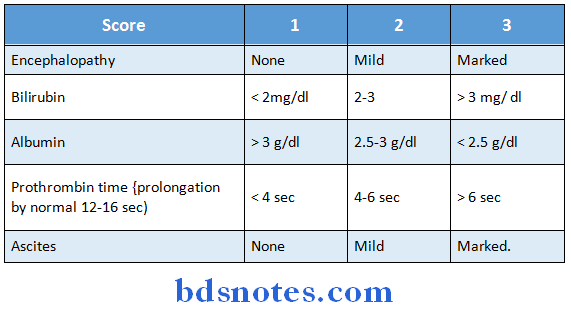
Child’s A-<7
B-7-9
C->9
Prognosis for ‘C’ is worst.
Leave a Reply