Pulpitis And Its Sequelae: From Inflammation To Bone Response
Question 1. Classify pulpitis and write its sequelae. Write in short etiology, clinical features, roentgenographic features, histology with treatment and prognosis of Garre’s osteomyelitis.
Answer. Inflammation of pulp is called pulpitis.
Classification of Pulpitis
Reversible
- Symptomatic (acute)
- Asymptomatic (chronic).
“Role of bacterial infection in pulpitis”
Irreversible
- Acute – Abnormally responsive to cold
- Abnormally responsive to heat
- Chronic – Asymptomatic with pulp exposure
- Hyperplastic pulpitis
- Internal resorption.
“Impact of untreated cavities on pulpitis”
pulpitis
Garre’S Osteomyelitis
- It is also called as chronic osteomyelitis with proliferative periostitis or periostitis ossifies or Garre’s chronic non-suppurative sclerosing ostitis.
- Garre’s osteomyelitis represents a reactive periosteal osteogenesis in response to low grade infection or trauma.
Etiology
- Mild infection
- Chronic periapical abscess
- Infected periapical cyst
- Mechanical irritation in the jaw from dentures
- Chronic trauma in the jaw bone.
reversible pulpitis
“Role of antibiotics in managing pulpitis”
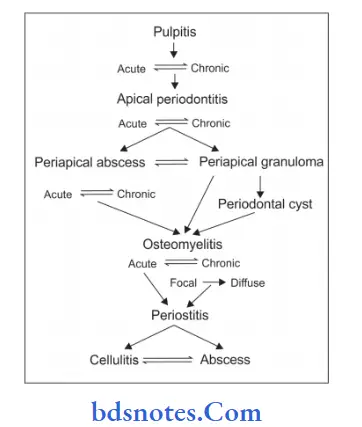
Sequelae Of Pulpitis
“Clinical examination for pulpitis”
Clinical Features
- It is common in young children and adults.
- Mandible is commonly involved in the posterior part.
- The involved jaw bone presents a carious nonvital tooth.
- There is a slight tenderness or a vague pain may be felt in the affected area of the bone.
- Slight pyrexia and leukocytosis may be present but ESR is normal.
Roentgenographic Features
- There is presence of a shadow of thin convex shell of bone over cortex.
- As the infection proceeds cortex become thick and laminated with alternating radiolucent and radiopaque layers. This is also known as onion skin appearance.
- Cancellous bone adjacent to the lesion can be normal, become sclerotic or it can show some areas of osteolytic changes.
- In the new bone osteolytic radiolucencies, i.e. small sequestra are seen.
“Global prevalence of pulpitis”
Histology
- There is presence of newly formed bone consisting of multiple osteoids and primitive bony tissue in sub periosteal region.
- Osteoblastic as well as osteoclastic activities are observed in central part of the bone.
- Marrow space contains firous tissues showing patchy areas of chronic inflammatory cell infiltration
- Trabeculae are oriented perpendicular to the cortex with trabeculae arranged, parallel to each other shows “retiform pattern”.
- Connective tissue between the bony trabeculae shows a diffuse or patchy sprinkling of lymphocytes and plasma cells.
“Treatment options for pulpitis”
Treatment And Prognosis
- Elimination of causative agent
- Extraction of carious infected tooth and antibiotic therapy
- Prognosis is good so no any additional surgical intervention is required.
Question 2. Describe etiopathogenesis of periapical granuloma.
Answer.
“Complications of untreated pulpitis”
Following is the etiopathogenesis of periapical granuloma:
- Periapical granuloma is caused as a response to prolonged irritation from infected root canals which leads to the extension of chronic apical periodontitis in PDL.
- Since pulp is infected it presents the release of inflammatory mediators such as prostaglandins,kinins and endotoxins. Elevated levels of IgG are seen in pulpoperiapical lesion.
- Inflammation as well as increase in the vascular pressure leads to abscess formation and resorption of bone in affcted area which is replaced by the granulation tissue.
Leave a Reply