Bone Loss And Patterns Of Bone Destruction
Describe the pathways of inflammation from gingiva to periodontal supporting tissues with appropriate diagrammatic presentation. Enumerate the various patterns of bone destruction in periodontitis and give a note on vertical or angular defects.
Answer.
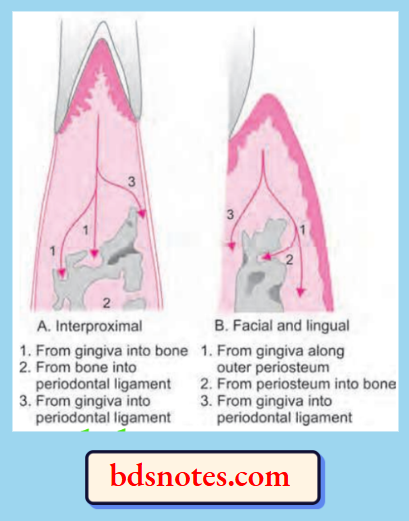
Pathways of Inflammation from Gingiva to Periodontal Supporting Tissues
- Interproximally from gingiva to bone and from bone to periodontal ligament.
- Facially and lingually from gingiva to bone along the outer bone and from gingiva into the periodontal ligament.
- Gingival inflammation can spread through transseptal fibers in the bone along the vessel channel which course throughout the alveolar bone and perforate the crest of interdental septum. The inflammation thus enters the centre of crest or through its side depending upon the course of the vessel channel. After reaching the bone, inflammation may again return to periodontal ligament.
- Gingival inflammation can spread directly from gingiva to periodontal ligament and from there on to interdental septum.
- Outer periosteal surface provides less physical resistance to spread of inflammation and inflammation thus spread lingually or facially along this surface and penetrate into the marrow spaces by coursing along supra periosteal vascular network.
Various Patterns of Bone Destruction in Periodontitis
- Horizontal bone loss
- Vertical or angular defects
- Osseous craters
- Bulbous bony contours
- Reverse architecture
- Ledges
- Furcation involvement.
- Fenestration and dehiscence
- Marginal gutter
- Irregular bony margins
Vertical or Angular Defects
Vertical or angular defects are those which occur in an oblique direction and leave a hollow out trough in bone alongside the root.
- Base of the defect is located apical to surrounding bone.
- Mostly angular defects are accompanied by intrabony periodontal pockets.
- Vertical defects detected radiographically appear most often on distal surfaces and mesial surfaces.
- When inflammation spread directly from gingiva to periodontal ligament and from periodontal ligament to bone it will lead to angular type of bone loss.
- Angular defects can also occur on facial and lingual or palatal surfaces, but these defects are not appreciated on the radiographs.
- Surgical exposure is the only means by which vertical osseous defects are detected.
- Vertical defects increases as the age advances.
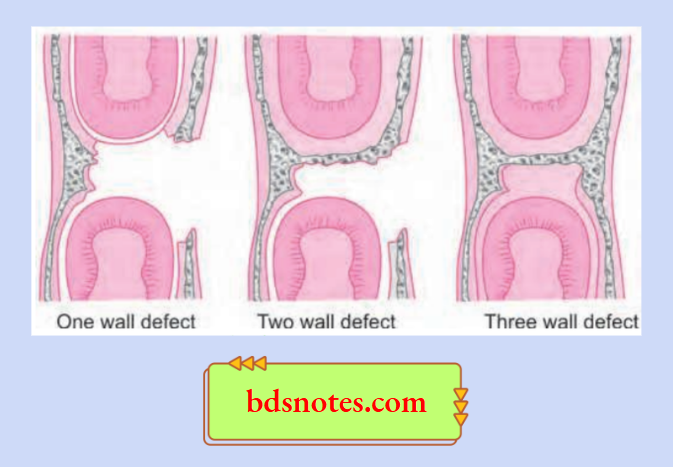
Classification of Vertical or Angular Defects
- One walled or hemiseptal defect: One wall is present
- Two walled defect: Two walls are present
- Three walled or intrabony defect: Three walls are present
- Combined osseous defect: Number of walls in apical portion of defect is greater than that in its occlusal portion. The less the number of walls remaining poor is the prognosis.
Leave a Reply