Tuberculous Lymphadenitis
Tubercular lymphadenitis is defied as chronic specific granulomatous inflammation with caseation necrosis of lymph node.
Causes of Cervical Lymphadenopathy
Inflammation and infection:
1. Bacterial infections:
Specific bacterial infection
- Tuberculosis
- Syphilis.
“Antibiotics For Tuberculous Lymphadenitis“
Non-specific bacterial infection
- Pericoronitis
- Periodontal disease
- Peri-apical infections.
Tuberculous Lymphadenitis
2. Viral infections:
- Infection mononucleosis
- AIDS
- Herpes simplex
- Cat scratch disease.

“Role Of Mycobacterium Tuberculosis In Tl”
3. Fungal infections:
- Oral candidiasis
- Histoplasmosis.
4. Parasitic infections:
- Rickettsial Infection.
Allergic conditions:
- Serum sickness.
Primary neoplasms:
- Lymphoma.
TB Lymphadenitis
“Risk Factors For Tuberculous Lymphadenitis”
Metastatic tumors:
- Oral squamous cell carcinoma
- Metastasis of carcinoma of breast.
Miscellaneous conditions:
- Leukemia
- Collagen diseases
- Sarcoidosis
- Non-tender lymphoid hyperplasia.
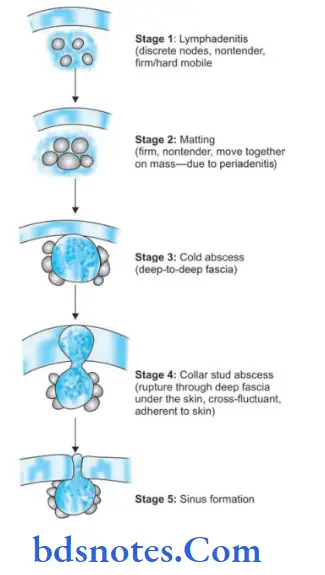
Tuberculous Lymphadenitis Staging
Stage of lymphadenitis
- Common in young adult between 20–30 years.
- Upper anterior deep cervical nodes are enlarged.
- Non-tender, discrete, mobile, fim lymph node is palpable.
Stage of Matting
- Results due to involvement of capsule of lymph node.
- Nodes moves together
- Firm, non-tender.
Stage of Cold abscess
- It occurs due to caseation necrosis of lymph node.
- No local rise in temperature.
- No tenderness.
- No redness.
- Soft, cystic and flctuant swelling.
- Transillumination is negative.
- On sternomastoid contraction test, it becomes less prominent indicating that it is deep-to-deep fascia.
Mycobacterium Tuberculosis Lymphadenitis
“Pathophysiology Of Tuberculous Lymphadenitis Explained”
Stage of Collar Stud abscess
It results when a cold abscess rupture through the deep fascia and form another swelling in the subcutaneous plane which is flctuant.
Stage of Sinus
- Collar stud abscess burst and form tubercular sinus.
- Common in young female.
- It can be multiple.
- Resemble an ulcer with undermined edge.
- No indurations.
- Skin surrounding the sinus shows pigmentation and sometimes bluish in color.
“Role Of Anti-Tb Drugs In Treating Tl”
“Treatment Options For Tuberculous Lymphadenitis”
Tuberculous Lymphadenitis Differential Diagnosis
- Non-specific lymphadenitis
- Secondaries in neck
- Lymphomas and chronic lymphatic leukemia
- Branchial cyst and lymphatic cyst mimic cold abscess
- HIV with lymph node involvement
Cervical Tuberculous Lymphadenitis
Tuberculous Lymphadenitis Investigations
- Hematocrit, ESR, peripheral smear.
- FNAC oflymph node and smear forAFB and culture: FNAC is very useful but not as superior as open node biopsy.
False negative, false positive results and altering the node architecture, and so eventual need of open biopsy are the problems.
Epithelioid cells (modifid histiocytes/macrophages) are diagnostic.
Langhans giant cells, lymphocytes, plasma cells are other features. - Open biopsy: Open biopsy is more reliable for tuberculosis (and also in lymphoma; but it is contraindicated in node secondaries); entire node ideally two nodes if possible has to be taken intact; one in formalin for pathology, other in normal saline for microbiology (AFB).
- HIV test (ELISA and western blot).
- Lowenstein-Jensen media is used for culture which takes 6 weeks to give result; so selenite media is often used which shows growth in 5 days.
- Mantoux test may be useful; but not very reliable.
- Chest X-ray to look for pulmonary tuberculosis.
- Polymerase chain reaction (PCR) is very useful method.
Leave a Reply