Bone Fractures: Types, Symptoms & Treatment
- Closed or simple fracture: When the outer skin is not injured due to the fracture. The fracture site does not communicate with the outer surface.
- Open or compound fracture: In this type, outer tissue is also broken down, and the fracture site communicates with the outer surface.
- Comminuted fracture: When the bone is broken down into more than two segments. It shows a bad prognosis.
- Impacted fracture: When one fragment enters another segment.
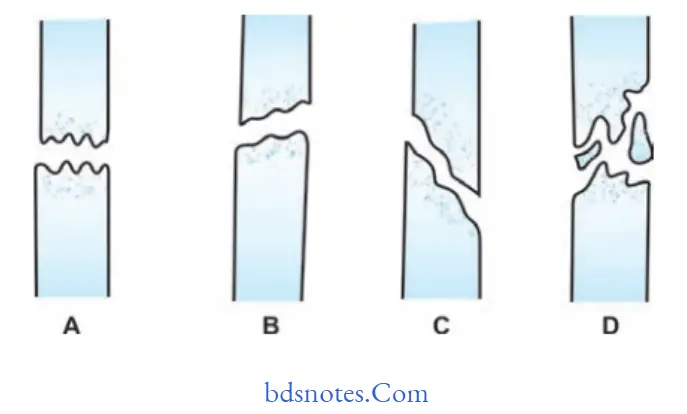
- Greenstick fracture: Only the bone is bent like a green stick.
- Fractures are incomplete and occur in children.
- Transverse, oblique, and spiral fractures.
- It depends upon the line of fracture.
- An oblique fracture shows a bad prognosis.
- Spiral fracture shows a good prognosis due to increased surface area.
- General Principles of Treatment of Fracture
- The three fundamental principles of fracture treatment are reduction, immobilization, preservation of function, and rehabilitation.
Bone Fracture
“Comminuted Fracture Recovery Time”
Read And Learn More: Maxillofacial Fractures, Disorders, and Treatments
- This first principle must be qualified by the words ‘if necessary’.
- In many fractures, reduction is unnecessary, either because there is no displacement or because the displacement is immaterial
- to the final result.
- If it is judged that perfect function can be restored without undue loss of time, despite some uncorrected displacement of the fragments, there is no object in striving for perfect anatomical reduction.
Indeed, meddlesome intervention may sometimes be detrimental, especially if it entails open operation.
- When reduction is decided upon it may be carried out in three ways:
- By closed manipulation
- By mechanical traction with or without manipulation
- By open operation.
Manipulative reduction
- Closed manipulation is the standard initial method of reducing the most common fractures. It is usually carried out under general anesthesia, but local or regional anesthesia is sometimes appropriate.
The technique is simply to grasp the fragments through the soft tissues, to disimpact them if necessary, and then to adjust them as nearly as possible to their correct position.
“Bone Fracture Healing Exercises”
Reduction By Mechanical Traction
- When the contraction of large muscles exerts a strong displacing force, some mechanical aid may be necessary to draw the fragments out to the normal length of the bone.
- This particularly applies to fractures of the shaft of the femur and certain types of fractures or displacement of the cervical spine.
- Traction may be applied either by weights or by a screw device, and the aim may be to gain full reduction rapidly at one sitting with anesthesia or to rely upon gradual reduction by prolonged traction without anesthesia.
Operative Reduction
Open reduction may also be required for some fractures involving articular surfaces or when the fracture is complicated by damage to a nerve or artery.
When operative reduction is resorted to, the opportunity should always be taken to fill the fragments internally to ensure that the position is maintained.
Immobilization
Indications For Immobilization
There are only three reasons for immobilizing a fracture:
Fracture Healing Process
3. To relieve pain.
- When immobilization is deemed necessary, there are four methods by which it may be achieved
- By a plaster of Paris cast or other external splint
- By continuous traction
- By external fixation
- By internal fixation.
- Immobilization by plaster, splint, or brace.
- For most fractures, the standard method of immobilization is by a plaster of Paris cast.

Plaster technique
The plaster bandages are applied in two forms: round-and round bandages and longitudinal strips or ‘slabs’ to reinforce a particular area.
Round-and-round bandages must be applied smoothly without tension, the material being drawn out to its full width at each turn. Slabs are prepared by unrolling a bandage to and fro upon a table; an average slab consists of about 12 thicknesses.
The slabs are placed at points of weakness or stress and are held in place by further turns of plaster bandage.
A plaster is best dried simply by exposure to the air: artificial heating is unnecessary.
Stress Fracture
Individual splints may also be made from malleable strips of aluminum, from wire, or heat-moldable plastic
This consists of a metal ‘halo’ or ring that is screwed to the skull and joined by bars to a plaster or plastic splint enclosing the chest.
Cast bracing (functional bracing): A brace has come to be understood as a supportive device that allows the continued function of the part.
Cast bracing, or functional fracture bracing (to use a better term), is a technique in which a fractured long bone is supported externally by plaster of Paris or by a mouldable plastic material in such a way that the function of the adjacent joints is preserved and use of the limb for its normal purposes can be resumed. Functional bracing is used mainly for fractures of the shaft of the femur or tibia.
“Types of Wrist Fractures”
Can A Bone Fracture Cause Permanent Disability?
Immobilization By Sustained Traction
This is particularly so when the plane of the fracture is oblique or spiral, because the elastic pull of the muscles, then tends to draw the distal fragment proximally so that it overlaps the proximal fragment.
In such a case, the pull of the muscles must be balanced by sustained traction upon the distal fragment, either by weight or by some other mechanical device.
Immobilization By External Fixation
- Strictly, immobilization in plaster or in a splint might be regarded as external fixation.
- By convention, however, the term external fixation is used to imply anchorage of the bone fragments to an external device such as a metal bar through the medium of pins inserted into the proximal and distal fragments of a long bone fracture.
- In its simplest form, external fixation may be provided by transfixing each fragment with a Steinmann pin and incorporating the protruding ends of the pins in a plaster of Paris splint.
- This simple method is now seldom used, and fiction is now using rigid bars or a frame.
Hairline Fracture
- Metal plate held by screws or locking plate (with screws fixed to the plate by threaded holes)
- Intramedullary nail, with or without cross-screw fixation for locking
- Dynamic compression screw-plate
- Condylar screw-plate
- Tension band wiring
- Transfiion screws.
Locking plate: A newer concept is the ‘locking plate’, which uses screws with heads that are threaded and when tightened lock into matching threads in the holes of the plate.
- This produces a more rigid fixation in terms of length and angle, which is particularly valuable in comminuted fractures in osteoporotic bone.
- It can also be inserted with less stripping of soft tissue that preserves bone vascularity, particularly in the metaphyseal region.
The screw component, which grips the femoral head, slides telescopically in the barrel to allow the bone fragments to be compressed together across the fracture. This compression effect is brought about by tightening a screw in the base of the barrel.
Kirschner wire fixation: These thin flexible wires with sharpened ends are available in several diameters and provide a useful alternative to transfusion screws for the fixation of small bony fragments or for fractures of the small bones in the hand and foot.
“Symptoms of a Buckle Fracture”
Types Of Fractures In Children And Their Treatments
Tension band wiring: This technique of fixation is most commonly used in the patella and olecranon, but can be applied to other small metaphyseal fragments such as the medial malleolus. It uses the mechanical principle of converting the tensile stresses of the muscles acting on the bone fragment, into a compressive force at the fracture site.
- Improved results in the treatment of fractures owe much to rehabilitation, perhaps the most important of the three great principles of fracture treatment.
- Reduction is often unnecessary; immobilization is often unnecessary; rehabilitation is always essential.
- Rehabilitation should begin as soon as the fracture comes under definitive treatment.
- Its purpose is twofold: first, to preserve functions of areas possible while the fracture is uniting, and second, to restore function to normal when the fracture is united.
- This purpose is achieved not so much by any passive treatment as by encouraging patients to help themselves.
- The two essential methods of rehabilitation are active use and active exercise.
- This implies that the patient must continue to use the injured part as naturally as possible within the limitations imposed by necessary treatment.
- The degree of function that can be retained depends upon the nature of the fracture, the risk of displacement ofthe fragments, and the extent of any necessary splintage.
- Although in some injuries rest may be necessary in the early days or weeks, there should be a graduated return to activity as soon as it can be allowed without risk.
- These comprise exercises for the muscles and joints. They should be encouraged from an early stage. While a limb is immobilized
- In plaster or splint, exercises must be directed mainly to the preservation of muscle function by static contractions.
- The ability to contract a muscle without moving a joint is soon acquired under proper supervision.
- When restrictive splints are no longer required, exercises should be directed to mobilizing the joints and building up the power of the muscles.
- Finally, when the fracture is soundly united, treatment may be intensified, movements being carried out against gradually increased resistance until normal power is regained.
Hematoma and granulation tissue formation
- After the fracture, a hematoma is formed due to the rupture of blood vessels
- Inflammatory changes start at the site of fracture
- Hematoma is gradually resorbed
- The necrotic debris is removed by neutrophils and macrophages
- Collagen fibers are laid down at the site of the union of fracture
- Capillaries and collagen fier form granulation tissue which covers the fracture site, it takes about 15 days
- Bone ends are now united at the fracture site, by a weak fibrous band.
Physical Therapy Exercises For Bone Fracture Recovery
- Calcification of newly formed fibrous tissue takes place after 3 weeks
- Matrix becomes ossified and is called ‘Callous’
- Callous is distributed along the fractured site
- Callous provides a firm and rigid bridge at the fracture segments.
- The callus is now replaced by a lamellar bone. The bone undergoes remodeling and comes in normal morphology
- The haversian system develops in the bone
- Bony union takes place in about 2 to 3 months.
Leave a Reply