Spirochetes
Question 1. Write a short note on the RPR test.
Answer:
Rapid Plasma Reagin (RPR):
“Understanding spirochetes through FAQs: Q&A explained”
The RPR test is the most popular. The RPR test uses the VDRL antigen containing fine carbon particles, which makes the result more clear-cut and more evident to the naked eye.
The RPR test can be done with unheated serum or plasma but is not suitable for testing CSF. Automated RPR test is available for large-scale tests.
An automated VDRL-ELISA test has been developed which can measure IgG and IgM antibodies separately and is suitable for large-scale testing of sera.
“Steps to explain types of spirochetes: Treponema vs Borrelia vs Leptospira: Q&A guide”
Biological false positive (BFP) reactions are defied as posi- reactions obtained in cardiolipin tests with negative results in specific treponemal tests, in the absence of past or present treponemal infections, and not caused by technical faults.
Reagin antibody becomes detectable 7–10 days after the appearance of the primary chancre. The sensitivity in the primary stage is 60-75% with the titers being low up to eight. In the secondary stage, the sensitivity is 100% and titers range from 16 to 128 or more. The prozone phenomenon may be a problem in high titer sera, and it is, therefore, essential to test sera in dilutions.
After the secondary stage, titers diminish and about a third of patients with late syphilis are seronegative. The titers may rise in patients developing cardiovascular, neurological, and gummatous lesions.
“Role of corkscrew motility in spirochete pathogenicity: Questions answered”
Read And Learn More: Microbiology Question And Answers
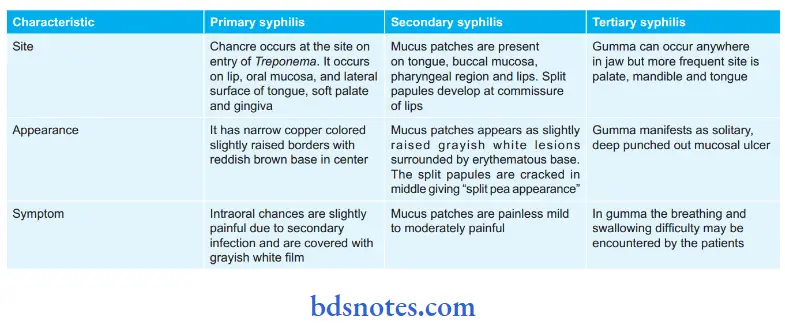
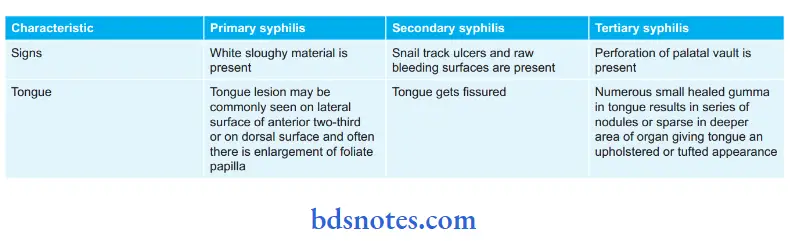
Question 2. Write a short note on oral lesions in syphilis.
Answer:
Following are the oral lesions in syphilis as per their stages:
“Importance of studying spirochetes for microbiology students: Questions explained”
“Common challenges in understanding spirochetes effectively: FAQs provided”
Question 3. Write a short answer on the oral manifestation of congenital syphilis.
Answer:
The following are the oral manifestations of congenital syphilis:
- The crown of the first molar in congenital syphilis is irregular and the enamel over an occlusal surface is arranged in an agglomerate mass of globules rather than a well-formed cusp.
- The crown gets constricted towards the incisal edge, leading to a screwdriver or peg-shaped incisor.
- In molars, positioning of the cusp towards the central portion of the crown gives a tooth bud shape or shrunken occlusal form known as mulberry molars or Moon’s molars.
- Affected molars are dirty yellow in color because of hypo calcification.
- The accessory monolingual cusp of a maxillary molar, i.e. clarabella cusp, is very prominent.
- Maxilla becomes hypoplastic and short, with relative mandibular prognathism.
- There is retarded root resorption of deciduous dentition.
“Factors influencing success with spirochete knowledge: Q&A”
- Marring of permanent incisors is seen in congenital syphilis.
- There is spacing present between cuspids and incisors.
- Malocclusion and open bite in present.
- There is the presence of linear scars which are radially arranged and perpendicular to a mucocutaneous junction, they are prominent over the lower lip near the angle of mouth.
- Post-rhagadic scars are the linear lesions present around oral orifices.
- They appear as red or copper-colored linear areas which are covered by the soft crust.
- Rhagades are more frequent over the lower lip
Leave a Reply